

CADASIL: Migraine, Encephalopathy, Stroke and Their Inter-Relationships
- PMID: 27309730
- PMCID: PMC4911105
- DOI: 10.1371/journal.pone.0157613
CADASIL: Migraine, Encephalopathy, Stroke and Their Inter-Relationships
Abstract
Background: Migraine is common in Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL) but its treatment responses are not well described, and its relationship to stroke risk unknown. Encephalopathy is a less common presentation; it has been suggested it is related to migraine. We characterised migraine patterns and treatment responses in CADASIL, and examined associations between migraine and both stroke risk and encephalopathy.
Methods: 300 symptomatic CADASIL patients were prospectively recruited from a national referral clinic over a nineteen year period, from 1996 to 2015. Data was collected using a standardised questionnaire. Migraine was classified according to the International Classification of Headache Disorders, 3rd edition (beta version). A cross-sectional analysis was carried out on the data collected.
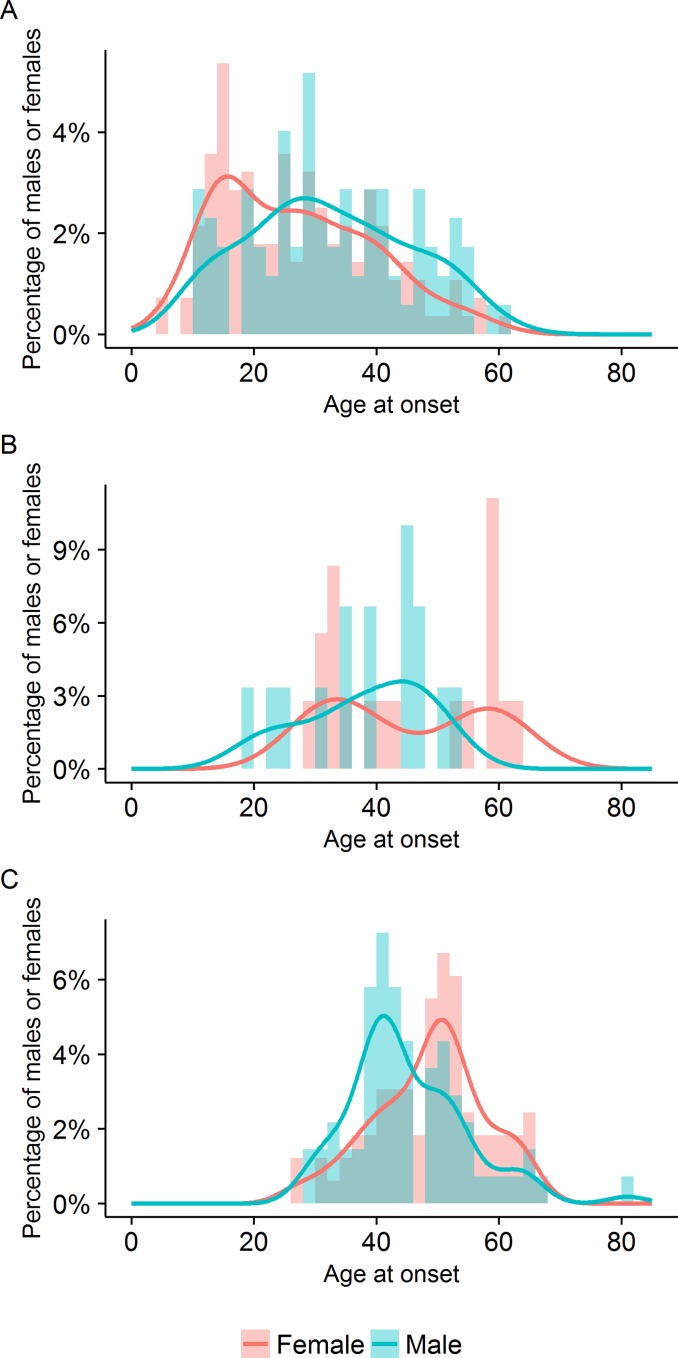
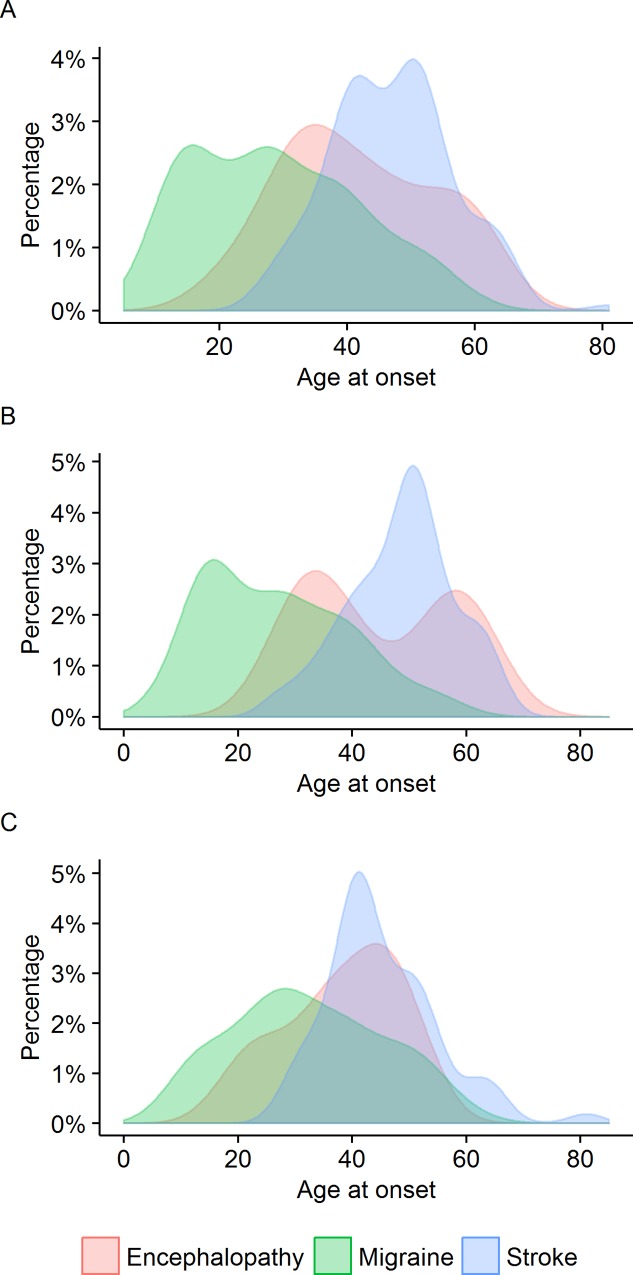
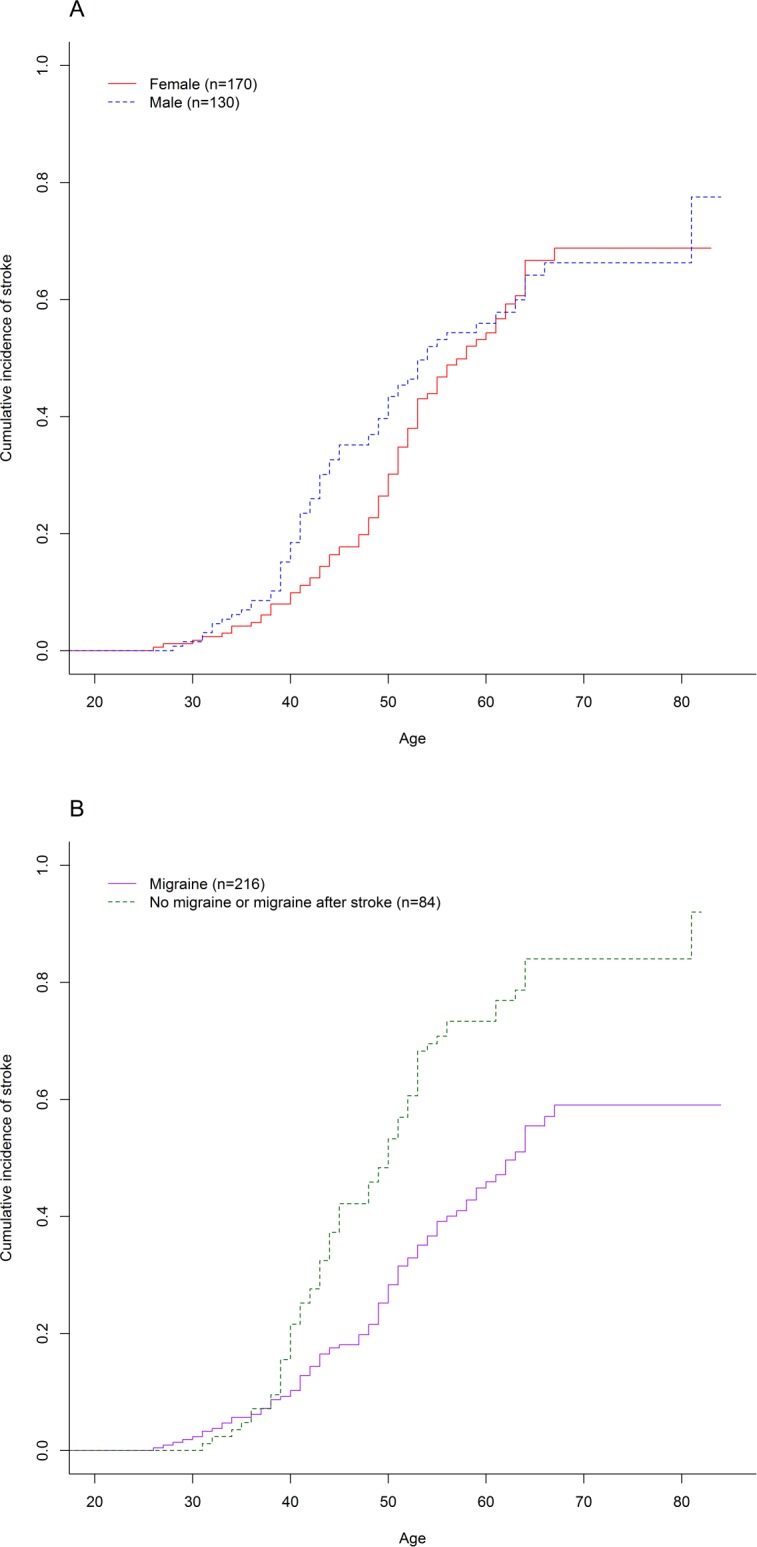
Results: Migraine was present in 226 (75.3%), and the presenting feature in 203 (67.7%). It was usually accompanied by aura (89.8%). Patients showed variable responses to a variety of drugs for migraine. Of 24 given triptans, 45.5% had consistent or partial responses. None had complications following triptans. Thirty-three (11.0%) patients experienced encephalopathy lasting on average 8.1 ± 3.4 days. Patients with migraine with aura had higher odds of encephalopathy (OR = 5.4; 95%CI 1.6-28.4; p = 0.002). Patients with confusional aura had higher odds of encephalopathy than those with other aura types (OR = 2.5, 95%CI = 1.0-5.8, p = 0.04). There was also no increase in risk of encephalopathy with sex or age at onset of migraine. Migraineurs had a lower stroke risk than non-migraineurs (HR = 0.46, 95%CI 0.3-0.6, p = 2.1x10-6).
Conclusions: Migraine with aura is a prominent feature of CADASIL. Treatment responses are similar to those seen in the general migraine population and no complications were observed with triptans. Migraine with aura was associated with increased risk of encephalopathy suggesting they may share pathophysiological mechanisms. There was no increased stroke risk associated with migraine, but risk appeared to be reduced although this finding needs confirming.
Conflict of interest statement
Figures
References
-
- Desmond DW, Moroney JT, Lynch T, Chan S, Chin SS, Mohr JP. The natural history of CADASIL: a pooled analysis of previously published cases. Stroke. 1999;30: 1230–3. Available: http://www.ncbi.nlm.nih.gov/pubmed/10356105 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
