

Association of the Extent of Resection With Survival in Glioblastoma: A Systematic Review and Meta-analysis
- PMID: 27310651
- PMCID: PMC6438173
- DOI: 10.1001/jamaoncol.2016.1373
Association of the Extent of Resection With Survival in Glioblastoma: A Systematic Review and Meta-analysis
Abstract
Importance: Glioblastoma multiforme (GBM) remains almost invariably fatal despite optimal surgical and medical therapy. The association between the extent of tumor resection (EOR) and outcome remains undefined, notwithstanding many relevant studies.
Objective: To determine whether greater EOR is associated with improved 1- and 2-year overall survival and 6-month and 1-year progression-free survival in patients with GBM.
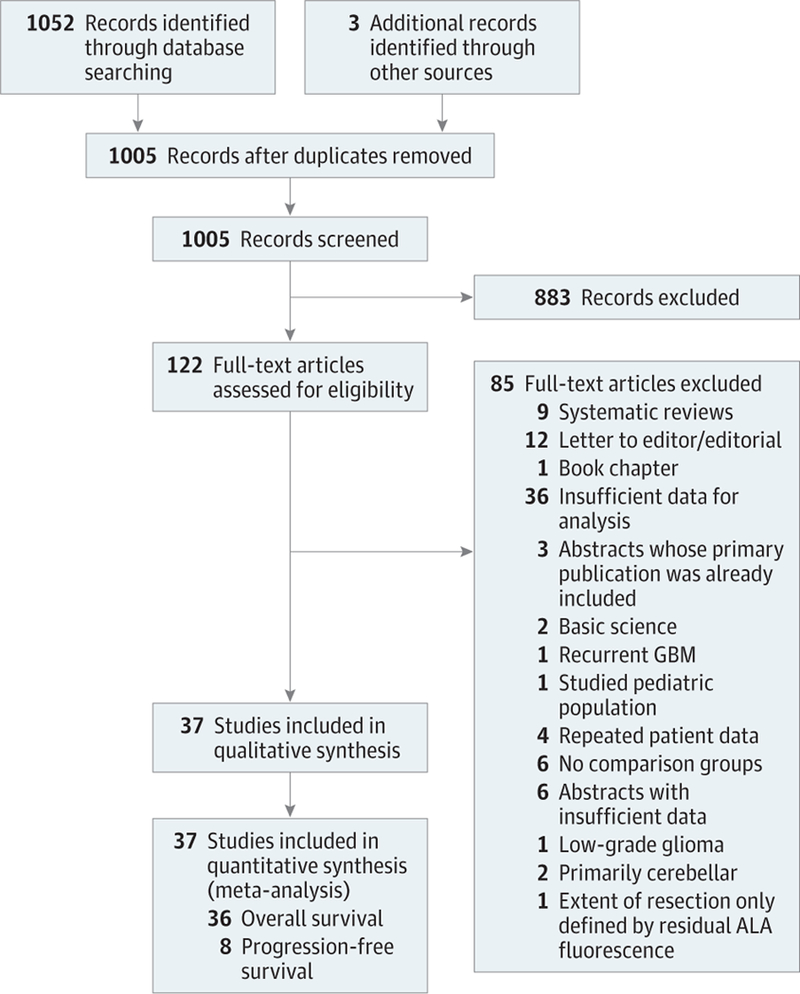
Data sources: Pubmed, CINAHL, and Web of Science (January 1, 1966, to December 1, 2015) were systematically reviewed with librarian guidance. Additional articles were included after consultation with experts and evaluation of bibliographies. Articles were collected from January 15 to December 1, 2015.
Study selection: Studies of adult patients with newly diagnosed supratentorial GBM comparing various EOR and presenting objective overall or progression-free survival data were included. Pediatric studies were excluded.
Data extraction and synthesis: Data were extracted from the text of articles or the Kaplan-Meier curves independently by investigators who were blinded to each other's results. Data were analyzed to assess mortality after gross total resection (GTR), subtotal resection (STR), and biopsy. The body of evidence was evaluated according to Grading of Recommendations Assessment, Development, and Evaluation (GRADE) criteria and PRISMA guidelines.
Main outcome and measures: Relative risk (RR) for mortality at 1 and 2 years and progression at 6 months and 1 year.
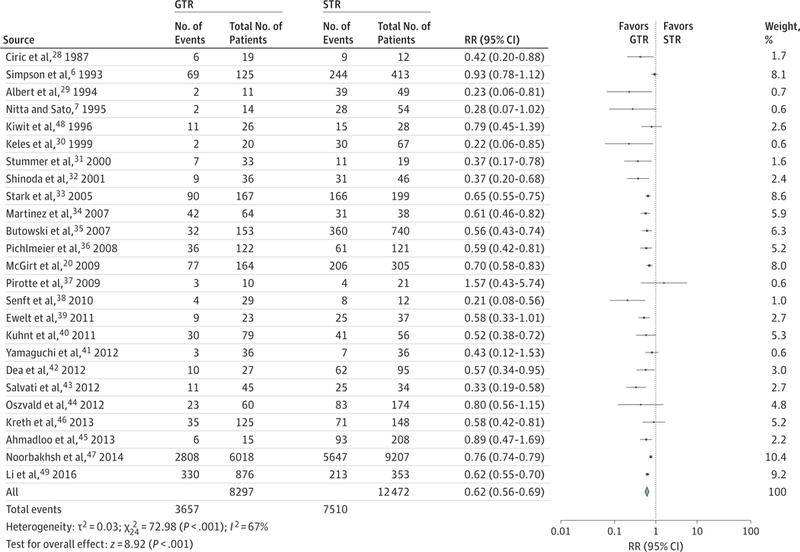
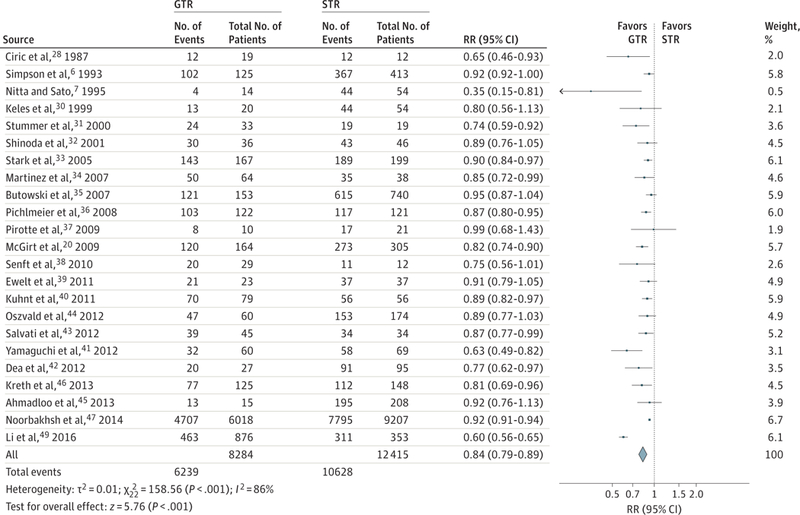
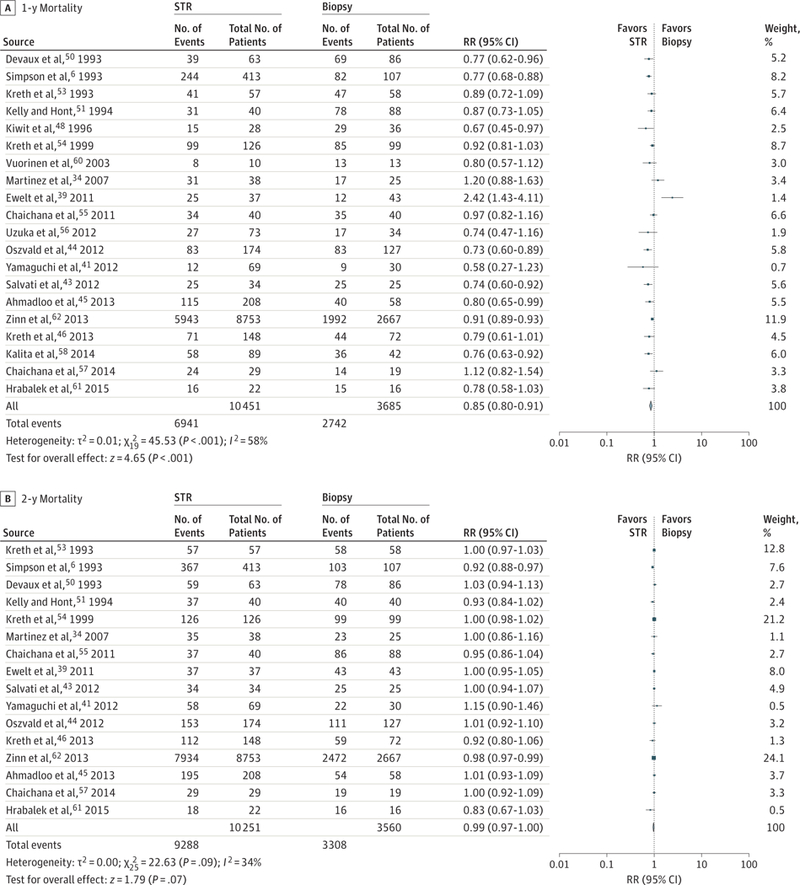
Results: The search produced 37 studies suitable for inclusion (41 117 unique patients). The meta-analysis revealed decreased mortality for GTR compared with STR at 1 year (RR, 0.62; 95% CI, 0.56-0.69; P < .001; number needed to treat [NNT], 9) and 2 years (RR, 0.84; 95% CI, 0.79-0.89; P < .001; NNT, 17). The 1-year risk for mortality for STR compared with biopsy was reduced significantly (RR, 0.85; 95% CI, 0.80-0.91; P < .001). The risk for mortality was similarly decreased for any resection compared with biopsy at 1 year (RR, 0.77; 95% CI, 0.71-0.84; P < .001; NNT, 21) and 2 years (RR, 0.94; 95% CI, 0.89-1.00; P = .04; NNT, 593). The likelihood of disease progression was decreased with GTR compared with STR at 6 months (RR, 0.72; 95% CI, 0.48-1.09; P = .12; NNT, 14) and 1 year (RR, 0.66; 95% CI, 0.43-0.99; P < .001; NNT, 26). The quality of the body of evidence by the GRADE criteria was moderate to low.
Conclusion and relevance: This analysis represents the largest systematic review and only quantitative systematic review to date performed on this subject. Compared with STR, GTR substantially improves overall and progression-free survival, but the quality of the supporting evidence is moderate to low.
Conflict of interest statement
Figures
Comment in
-
Extent of Resection and Survival in Glioblastoma Multiforme.JAMA Oncol. 2016 Nov 1;2(11):1508-1509. doi: 10.1001/jamaoncol.2016.3806. JAMA Oncol. 2016. PMID: 27684297 No abstract available.
-
Extent of Resection and Survival in Glioblastoma Multiforme.JAMA Oncol. 2016 Nov 1;2(11):1509. doi: 10.1001/jamaoncol.2016.3809. JAMA Oncol. 2016. PMID: 27684359 No abstract available.
-
Extent of Resection and Survival in Glioblastoma Multiforme-Reply.JAMA Oncol. 2016 Nov 1;2(11):1509-1510. doi: 10.1001/jamaoncol.2016.3812. JAMA Oncol. 2016. PMID: 27684462 No abstract available.
-
Gross Total Resection of Glioblastoma Improves Overall Survival and Progression-Free Survival Compared to Subtotal Resection or Biopsy Alone.Neurosurgery. 2016 Dec;79(6):N12-N13. doi: 10.1227/01.neu.0000508600.08200.c1. Neurosurgery. 2016. PMID: 27861406 No abstract available.
References
-
- Stupp R, Mason WP, van den Bent MJ, et al.; European Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy Groups; National Cancer Institute of Canada Clinical Trials Group. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005;352(10):987–996. - PubMed
-
- Sanai N, Polley M-Y, McDermott MW, Parsa AT, Berger MS. An extent of resection threshold for newly diagnosed glioblastomas. J Neurosurg 2011; 115(1):3–8. - PubMed
-
- Aldave G, Tejada S, Pay E, et al. Prognostic value of residual fluorescent tissue in glioblastoma patients after gross total resection in 5-aminolevulinic acid–guided surgery. Neurosurgery 2013;72(6):915–920. - PubMed
-
- Lacroix M, Abi-Said D, Fourney DR, et al. A multivariate analysis of 416 patients with glioblastoma multiforme: prognosis, extent of resection, and survival. J Neurosurg 2001;95(2): 190–198. - PubMed
-
- Sanai N, Mirzadeh Z, Polley M-Y, Berger MS. The value of glioblastoma extent of resection: a volumetric analysis of 500 patients. J Neurosurg 2010;113(2):A433.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
