

STARD-compliant article: The utility of red cell distribution width to predict mortality for septic patients visiting the emergency department
- PMID: 27310948
- PMCID: PMC4998434
- DOI: 10.1097/MD.0000000000003692
STARD-compliant article: The utility of red cell distribution width to predict mortality for septic patients visiting the emergency department
Erratum in
-
Erratum: Medicine, Volume 95, Issue 24: Erratum.Medicine (Baltimore). 2016 Aug 7;95(31):e5074. doi: 10.1097/01.md.0000490009.39850.74. eCollection 2016 Aug. Medicine (Baltimore). 2016. PMID: 31265618 Free PMC article.
Abstract
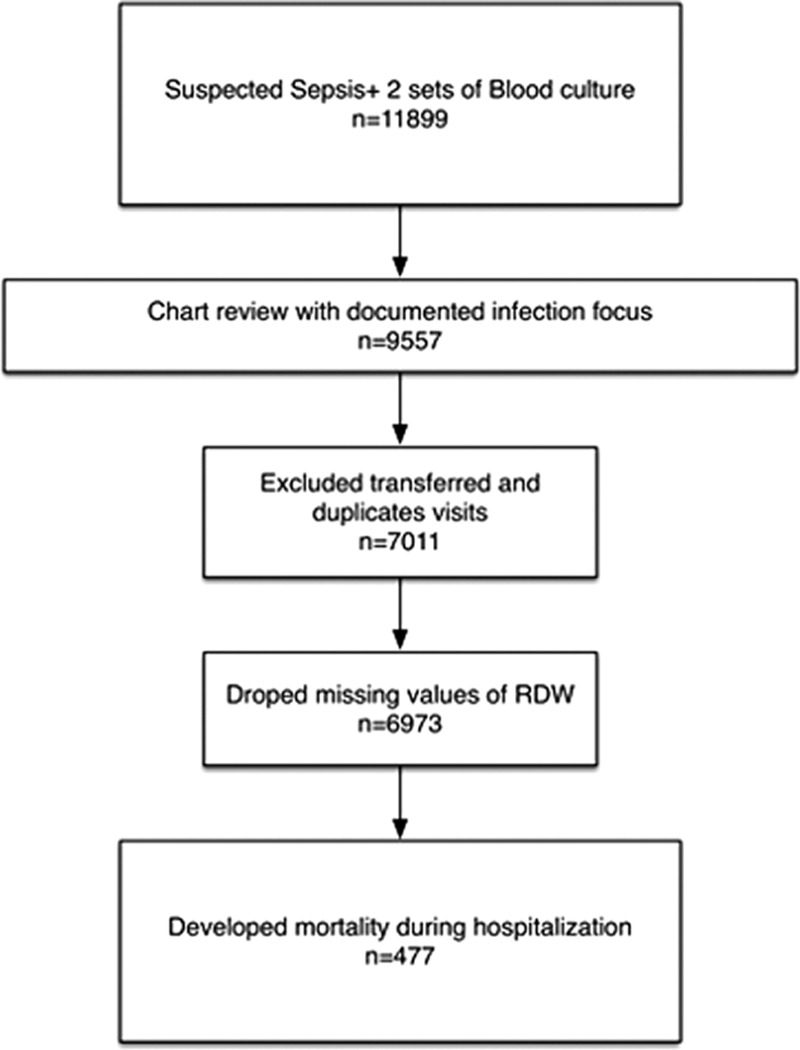
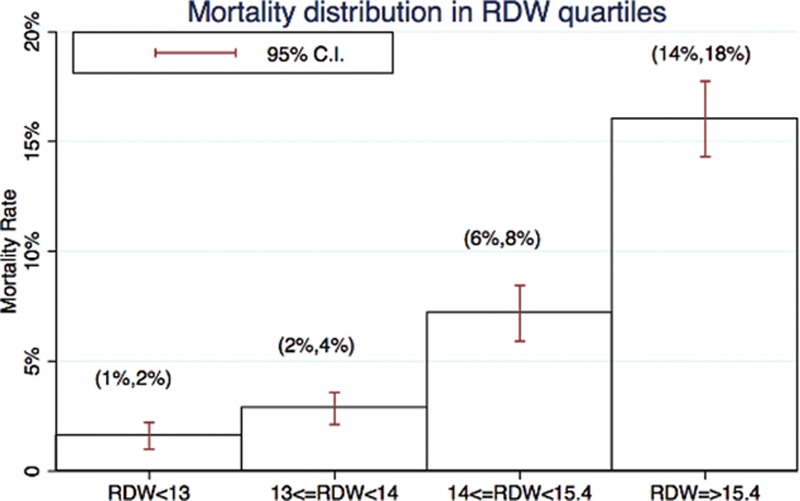
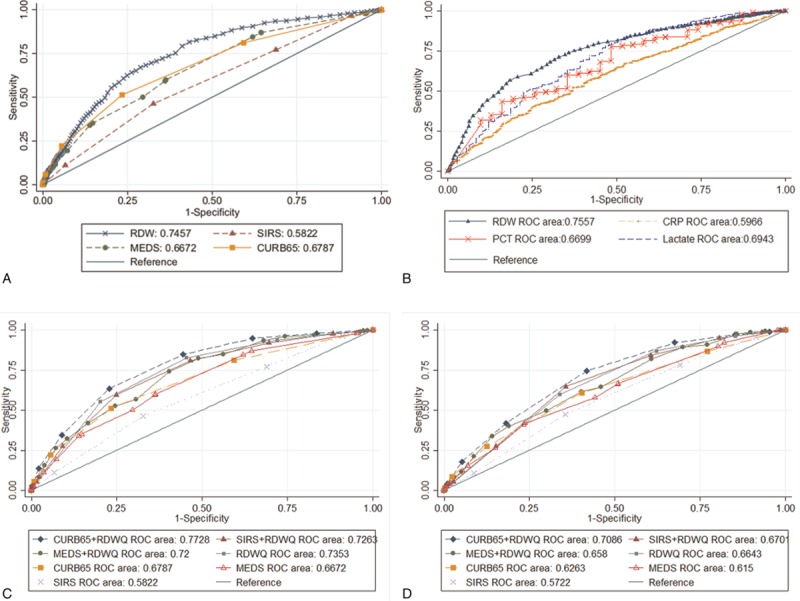
Sepsis is a common condition in the emergency department that is associated with high mortality. Red blood cell distribution width (RDW) has been used as a simple prognosis predictor for patients with community-acquired pneumonia, gram-negative bacteremia, and severe sepsis or septic shock. To evaluate the performance of RDW to predict in-hospital mortality among septic patients, we conducted a hospital-based retrospective cohort study in an emergency department of a tertiary teaching hospital. RDW was compared with other commonly used clinical prediction scores (Systemic Inflammatory Response Syndrome (SIRS), Mortality in Emergency Department Sepsis (MEDS) and the Confusion, Urea nitrogen, Respiratory rate, Blood pressure, 65 years of age and older (CURB65)). Of 6973 consecutive adult patients with a clinical diagnosis of sepsis and 2 sets of blood culture ordered by physicians, 477 (6.8%) died. The mortality group had higher RDW levels than the survival group (15.7% vs 13.8%). After dividing RDW into quartiles, the patients in the highest RDW quartile (RDW >15.6%; mortality, 16.7%) had more than twice the risk of in-hospital mortality compared with patients in the second highest quartile (RDW >14% and <15.6%; mortality, 7.3%), whereas the mortality rate in the lowest RDW quartile (<13.1%) was only 1.6%. The area under the receiver operating characteristic curve of RDW to predict mortality was 0.75 (95% confidence interval, 0.72-0.77), which is significantly higher than the areas under the curve of clinical prediction rules (SIRS, MEDS, and CURB65). After integrating RDW into these scores, all scores performed better in predicting mortality (0.73, 0.72, and 0.77, for SIRS, MEDS, and CURB65, respectively). RDW could be an independent predictor of mortality among septic patients. Clinicians could classify the septic patients into different risk groups according to RDW quartiles. For more accurate mortality prediction, RDW could be a potential parameter to be incorporated into clinical prediction rules.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Kaukonen KM, Bailey M, Pilcher D, et al. Systemic inflammatory response syndrome criteria in defining severe sepsis. N Engl J Med 2015;372:1629–38. - PubMed
-
- Shapiro NI, Wolfe RE, Moore RB, et al. Mortality in Emergency Department Sepsis (MEDS) score: a prospectively derived and validated clinical prediction rule. Crit Care Med 2003;31:670–5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
