

No differences in metabolic outcomes between nadir GH 0.4 and 1.0 ng/mL during OGTT in surgically cured acromegalic patients (observational study)
- PMID: 27310957
- PMCID: PMC4998443
- DOI: 10.1097/MD.0000000000003808
No differences in metabolic outcomes between nadir GH 0.4 and 1.0 ng/mL during OGTT in surgically cured acromegalic patients (observational study)
Erratum in
-
Erratum: Medicine, Volume 95, Issue 24: Erratum.Medicine (Baltimore). 2016 Aug 7;95(31):e5074. doi: 10.1097/01.md.0000490009.39850.74. eCollection 2016 Aug. Medicine (Baltimore). 2016. PMID: 31265618 Free PMC article.
Abstract
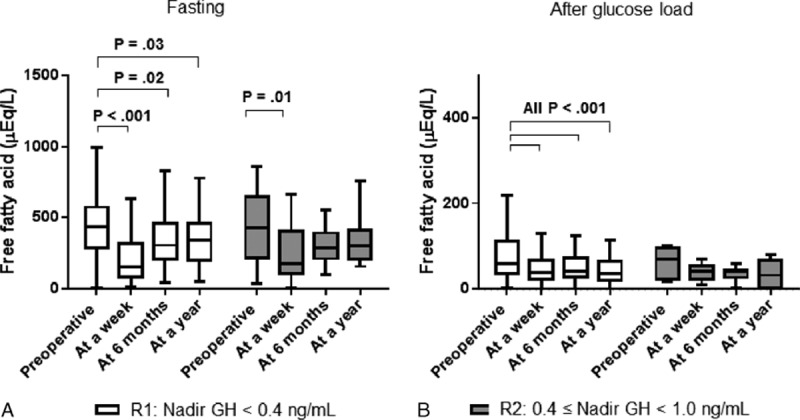
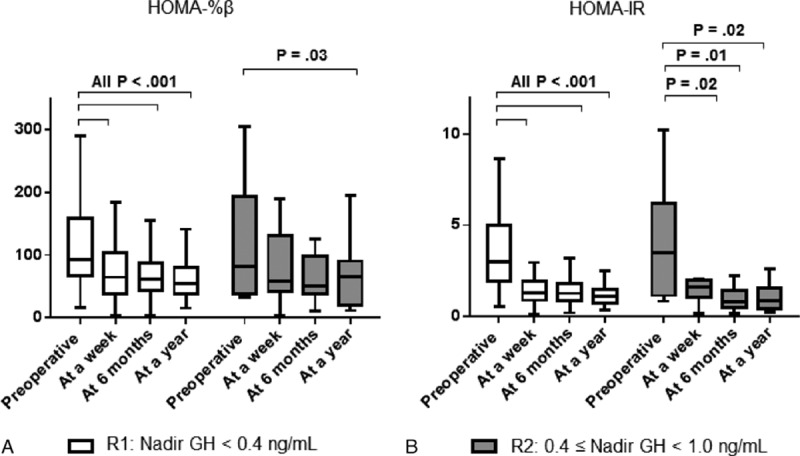
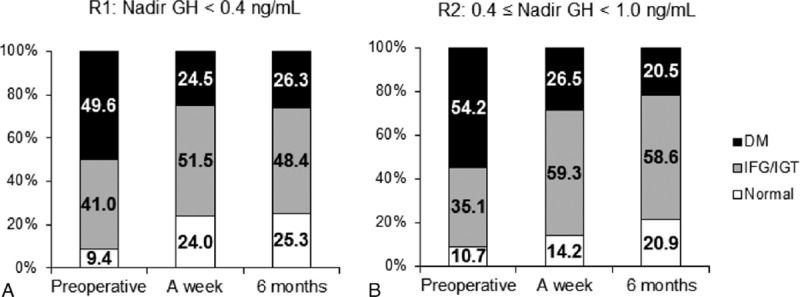
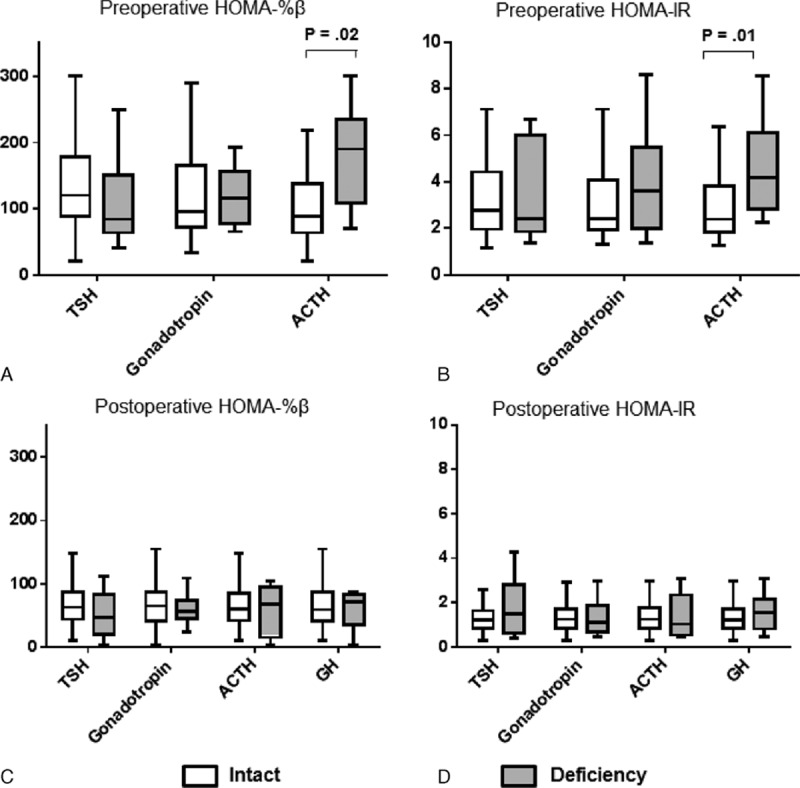
Metabolic impairment is the common cause for mortality in acromegalic patients. In this study, long-term improvements of metabolic parameters were evaluated according to 2 different remission criteria.This was an observational cohort study before and up to 1 year after transsphenoidal adenomectomy (TSA). Participants were 187 patients with acromegaly. At 6 months after TSA, remitted patients with age- and sex-matched normalized IGF-1 were divided into 2 groups: remission 1 (R1), nadir growth hormone (GH) below 0.4 ng/mL; and remission 2 (R2), nadir GH between 0.4 and 1.0 ng/mL in oral glucose tolerance test (OGTT). Metabolic parameters during serial OGTTs were evaluated for 12 months. Remission was achieved in 157 (R1-136; R2-21) patients. Immediate postoperative metabolic parameters including body weight, body mass index, glucose, insulin, and free fatty acid in OGTT were all significantly improved in R1 and R2. HOMA-%β and HOMA-IR scores also improved in both R1 and R2. These improvements persisted for duration (12 months) of this study. However, no difference was present in metabolic parameters between R1 and R2. Although the patients with preoperative adrenal insufficiency presented significantly increased HOMA scores before TSA, there was no difference between classifications of deficient pituitary axes and changes of metabolic parameters after TSA. Remitted patients exhibited rapid restoration of metabolic parameters immediate postoperative period. Long-term improvements in metabolic parameters were not different between the 2 different nadir GH cut-offs, 0.4 and 1.0 ng/mL.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Melmed S. Medical progress: acromegaly. N Engl J Med 2006;355:2558–73. - PubMed
-
- Holdaway IM, Rajasoorya RC, Gamble GD. Factors influencing mortality in acromegaly. J Clin Endocrinol Metab 2004;89:667–74. - PubMed
-
- Kasayama S, Otsuki M, Takagi M, et al. Impaired beta-cell function in the presence of reduced insulin sensitivity determines glucose tolerance status in acromegalic patients. Clin Endocrinol (Oxf) 2000;52:549–55. - PubMed
-
- M⊘ller N, J⊘rgensen JO. Effects of growth hormone on glucose, lipid, and protein metabolism in human subjects. Endocr Rev 2009;30:152–77. - PubMed
-
- Ciresi A, Amato MC, Pivonello R, et al. The metabolic profile in active acromegaly is gender-specific. J Clin Endocrinol Metab 2013;98:E51–59. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
