

The impact of surgical treatments for lower urinary tract symptoms/benign prostatic hyperplasia on male erectile function: A systematic review and network meta-analysis
- PMID: 27310968
- PMCID: PMC4998454
- DOI: 10.1097/MD.0000000000003862
The impact of surgical treatments for lower urinary tract symptoms/benign prostatic hyperplasia on male erectile function: A systematic review and network meta-analysis
Erratum in
-
Erratum: Medicine, Volume 95, Issue 24: Erratum.Medicine (Baltimore). 2016 Aug 7;95(31):e5074. doi: 10.1097/01.md.0000490009.39850.74. eCollection 2016 Aug. Medicine (Baltimore). 2016. PMID: 31265618 Free PMC article.
Abstract
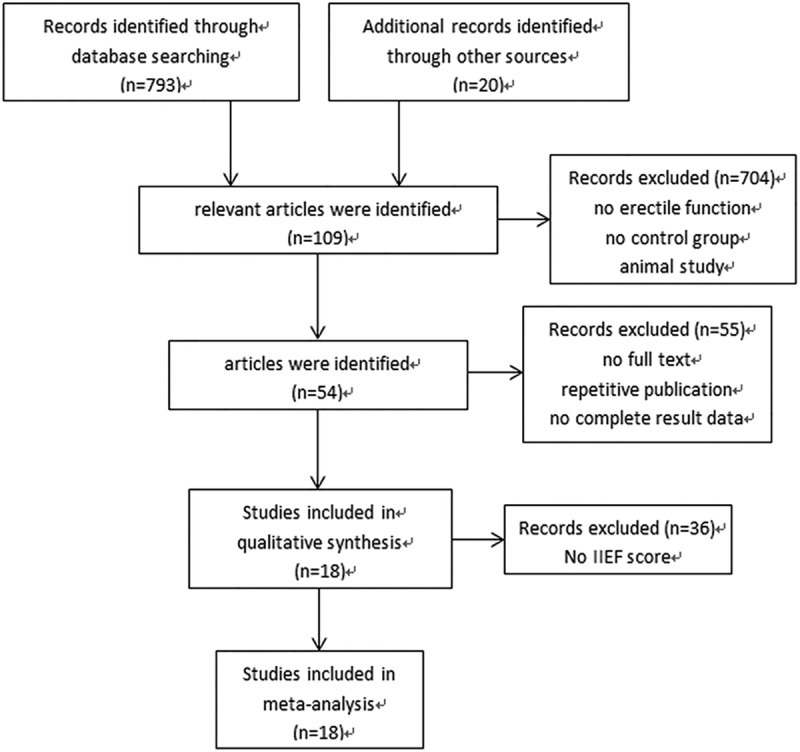
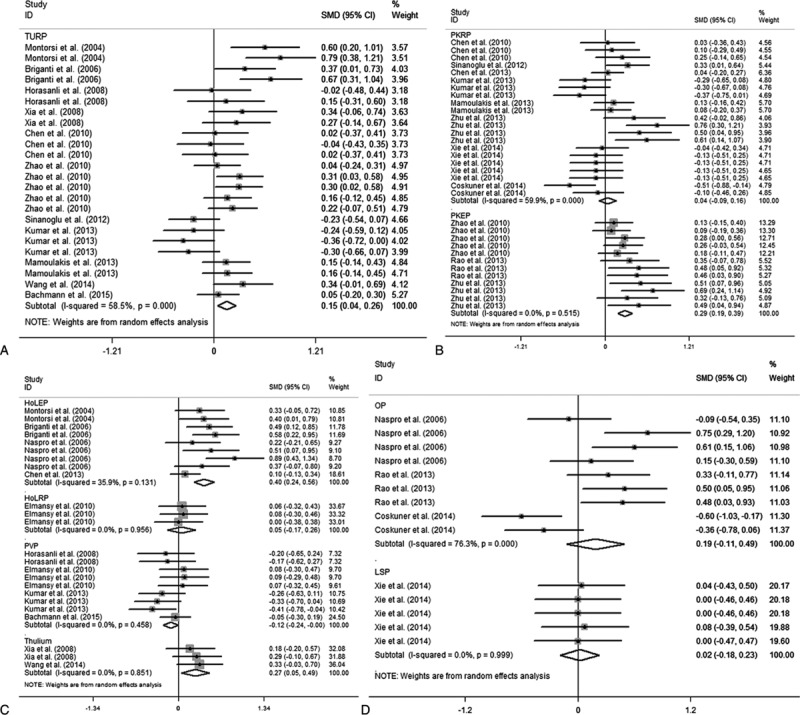
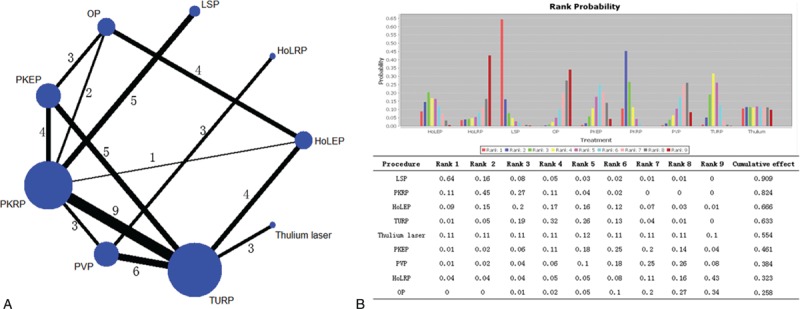
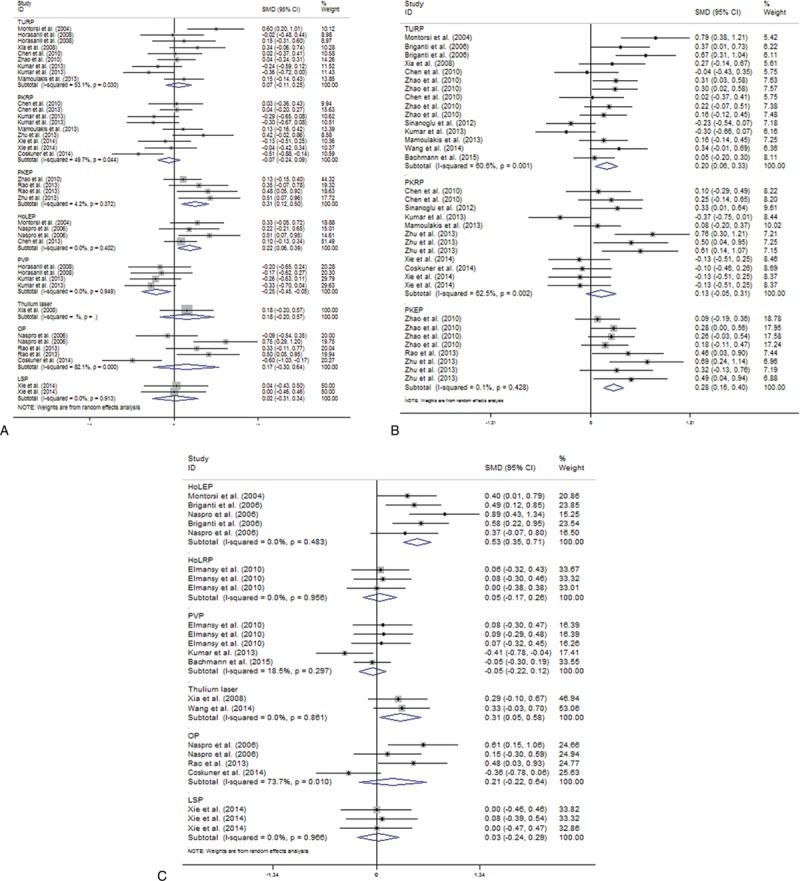
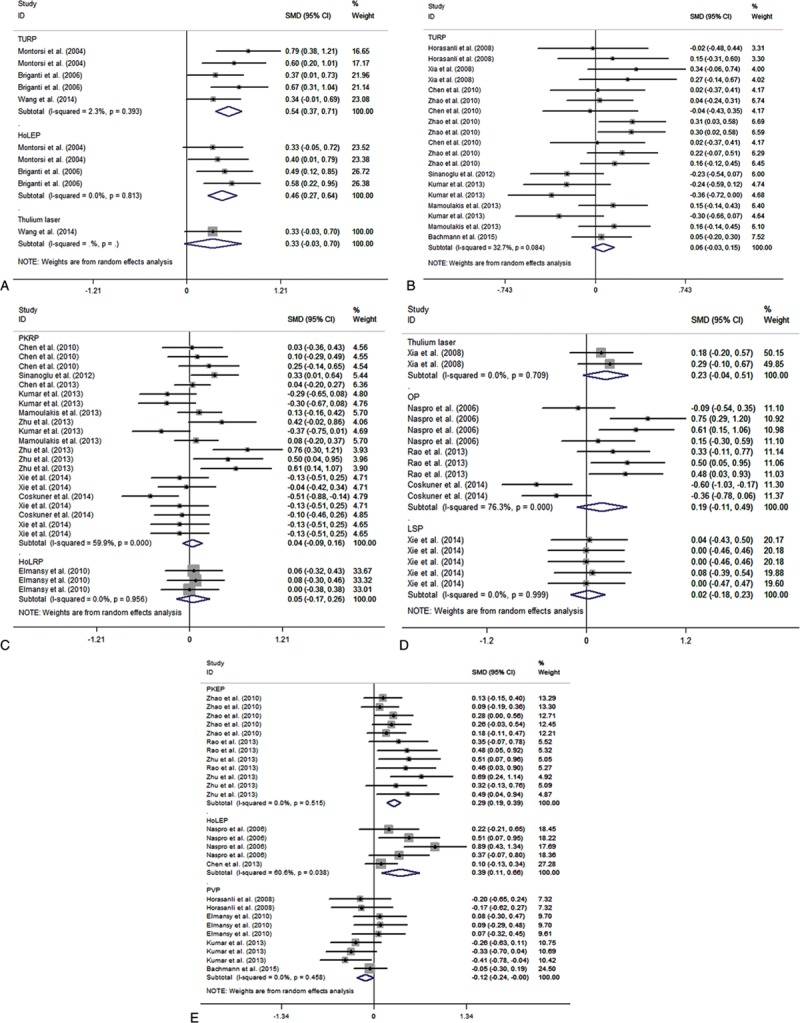
Lower urinary tract symptoms (LUTS)/benign prostatic hyperplasia (BPH) is common in adult men and can impair erectile function (EF). It was believed surgical treatments for this illness can improve EF due to the relief of LUTS while they were also reported harmed EF as heating or injury effect. Current network meta-analysis aimed to elucidate this discrepancy.Randomized controlled trials (RCTs) were identified. Direct comparisons were conducted by STATA and network meta-analysis was conducted by Generate Mixed Treatment Comparison. Random-effects models were used to calculate pooled standard mean difference and 95% confidence intervals and to incorporate variation between studies.Eighteen RCTs with 2433 participants were analyzed. Nine approaches were studied as transurethral resection of the prostate (TURP), plasmakinetic resection of the prostate (PKRP), plasmakinetic enucleation of the prostate (PKEP), Holmium laser enucleation of the prostate (HoLEP), Holmium laser resection of the prostate (HoLRP), photoselective vaporization of the prostate (PVP), Thulium laser, open prostatectomy (OP), and laparoscopic simple prostatectomy (LSP). In direct comparisons, all surgical treatments did not decrease postoperative International Index of Erectile Function (IIEF)-5 score except PVP. Moreover, patients who underwent HoLEP, PKEP, Thulium laser, and TURP had their postoperative EF significantly increased. Network analysis including direct and indirect comparisons ranked LSP at the highest position on the variation of postoperative IIEF-5 score, followed by PKRP, HoLEP, TURP, Thulium laser, PKEP, PVP, HoLRP, and OP. In subgroup analysis, only PVP was found lower postoperative EF in the short term and decreased baseline group, whereas TURP increased postoperative IIEF-5 score only for patients with normal baseline EF. However, HoLEP and PKEP showed pro-erectile effect even for patients with decreased baseline EF and short-term follow-up. Our novel data demonstrating surgical treatments for LUTS/BPH showed no negative impact on postoperative EF except PVP. Moreover, HoLEP and PKEP were found pro-erectile effect for all subgroups. New technologies, such as LSP, PKRP, and Thulium laser, were ranked at top positions in the network analysis, although they had no pro-erectile effect in direct comparison due to limited original studies or poor baseline EF. Therefore, further studies and longer follow-up are required to substantiate our findings.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Gratzke C, Bachmann A, Descazeaud A, et al. EAU guidelines on the assessment of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. Eur Urol 2015;67:1099–109. - PubMed
-
- Vuichoud C, Loughlin KR. Benign prostatic hyperplasia: epidemiology, economics and evaluation. Can J Urol 2015;22(5 suppl 1):1–6. - PubMed
-
- Garraway WM, Collins GN, Lee RJ. High prevalence of benign prostatic hypertrophy in the community. Lancet 1991;338:469–71. - PubMed
-
- Chute CG, Panser LA, Girman CJ, et al. The prevalence of prostatism: a population-based survey of urinary symptoms. J Urol 1993;150:85–9. - PubMed
-
- Sexton CC, Coyne KS, Kopp ZS, et al. The overlap of storage, voiding and postmicturition symptoms and implications for treatment seeking in the USA, UK and Sweden: EpiLUTS. Br J Urol Int 2009;103suppl 3:12–23. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
