

Swallowing dysfunction following endotracheal intubation: Age matters
- PMID: 27310972
- PMCID: PMC4998458
- DOI: 10.1097/MD.0000000000003871
Swallowing dysfunction following endotracheal intubation: Age matters
Erratum in
-
Erratum: Medicine, Volume 95, Issue 24: Erratum.Medicine (Baltimore). 2016 Aug 7;95(31):e5074. doi: 10.1097/01.md.0000490009.39850.74. eCollection 2016 Aug. Medicine (Baltimore). 2016. PMID: 31265618 Free PMC article.
Abstract
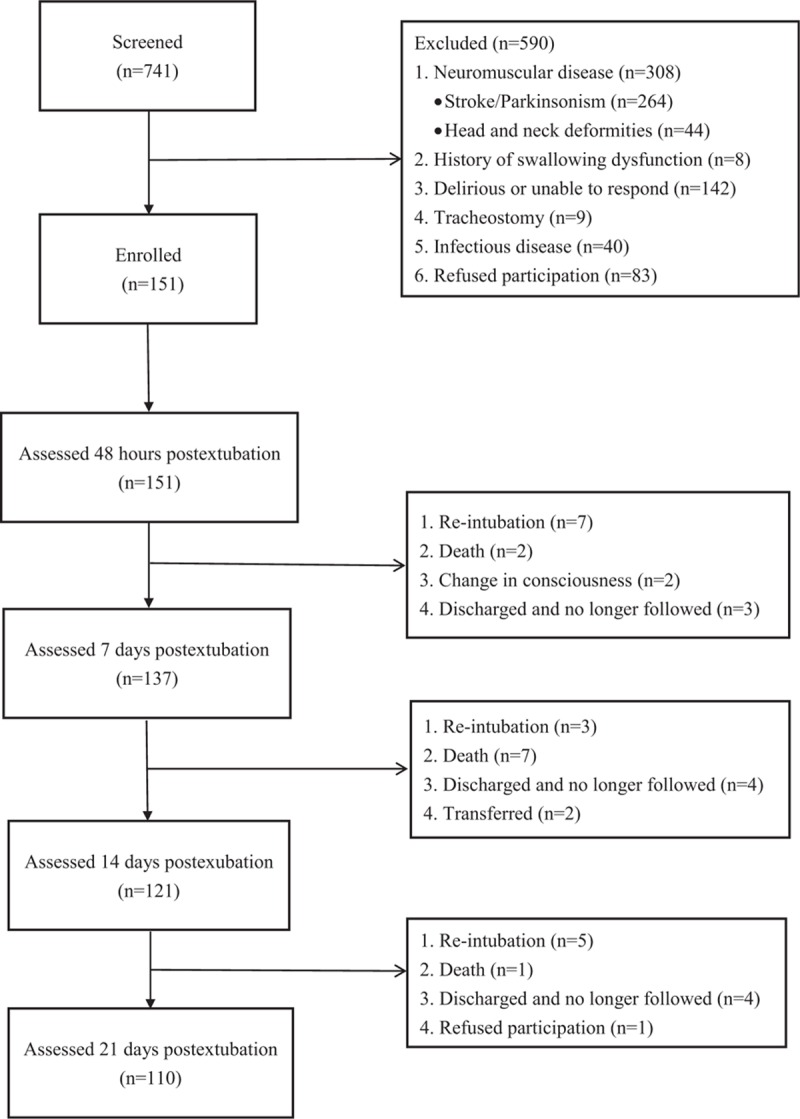
To evaluate postextubation swallowing dysfunction (PSD) 21 days after endotracheal extubation and to examine whether PSD is time-limited and whether age matters.For this prospective cohort study, we evaluated 151 adult critical care patients (≥20 years) who were intubated for at least 48 hours and had no pre-existing neuromuscular disease or swallowing dysfunction. Participants were assessed for time (days) to pass bedside swallow evaluations (swallow 50 mL of water without difficulty) and to resume total oral intake. Outcomes were compared between younger (20-64 years) and older participants (≥65 years).PSD, defined as inability to swallow 50 mL of water within 48 hours after extubation, affected 92 participants (61.7% of our sample). At 21 days postextubation, 17 participants (15.5%) still failed to resume total oral intake and were feeding-tube dependent. We found that older participants had higher PSD rates at 7, 14, and 21 days postextubation, and took significantly longer to pass the bedside swallow evaluations (5.0 vs 3.0 days; P = 0.006) and to resume total oral intake (5.0 vs 3.0 days; P = 0.003) than their younger counterparts. Older participants also had significantly higher rates of subsequent feeding-tube dependence than younger patients (24.1 vs 5.8%; P = 0.008).Excluding patients with pre-existing neuromuscular dysfunction, PSD is common and prolonged. Age matters in the time needed to recover. Swallowing and oral intake should be monitored and interventions made, if needed, in the first 7 to 14 days postextubation, particularly for older patients.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

References
-
- Bordon A, Bokhari R, Sperry J, et al. Swallowing dysfunction after prolonged intubation: analysis of risk factors in trauma patients. Am J Surg 2011;202:679–83. - PubMed
-
- de Larminat V, Montravers P, Dureuil B, et al. Alteration in swallowing reflex after extubation in intensive care unit patients. Crit Care Med 1995;23:486–90. - PubMed
-
- Skoretz SA, Flowers HL, Martino R. The incidence of dysphagia following endotracheal intubation. Chest 2010;137:665–73. - PubMed
-
- Skoretz S, Yau T, Ivanov J, et al. Dysphagia and associated risk factors following extubation in cardiovascular surgical patients. Dysphagia 2014;29:647–54. - PubMed
-
- Macht M, Wimbish T, Bodine C, et al. ICU-acquired swallowing disorders. Crit Care Med 2013;41:2396–405. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
