

Can S-1 replace fluorouracil for advanced gastric cancer? A PRISMA-compliant systematic review and meta-analysis
- PMID: 27310997
- PMCID: PMC4998483
- DOI: 10.1097/MD.0000000000003916
Can S-1 replace fluorouracil for advanced gastric cancer? A PRISMA-compliant systematic review and meta-analysis
Erratum in
-
Erratum: Medicine, Volume 95, Issue 24: Erratum.Medicine (Baltimore). 2016 Aug 7;95(31):e5074. doi: 10.1097/01.md.0000490009.39850.74. eCollection 2016 Aug. Medicine (Baltimore). 2016. PMID: 31265618 Free PMC article.
Abstract
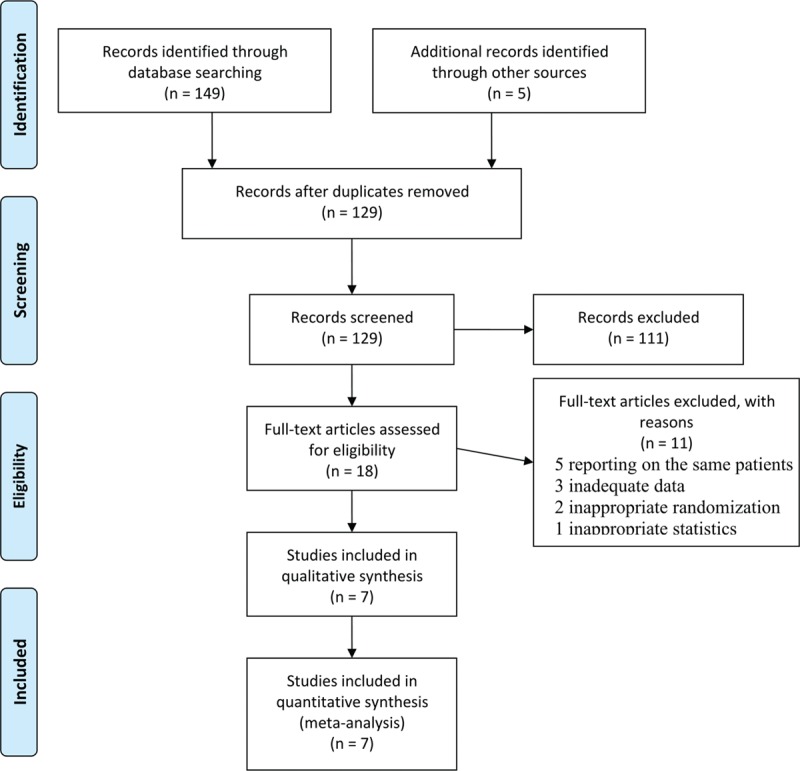
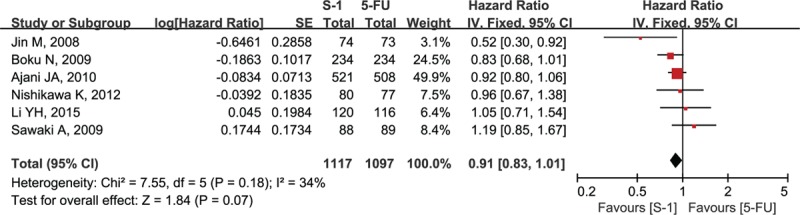
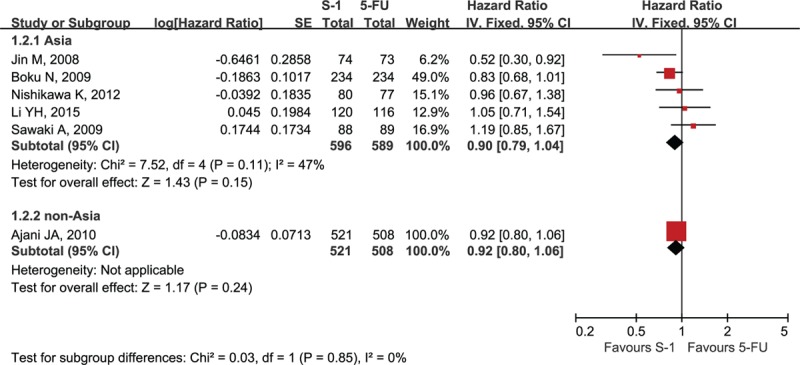
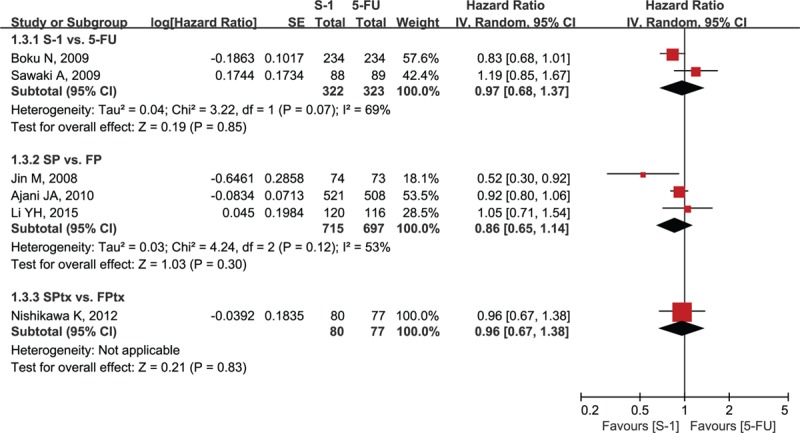
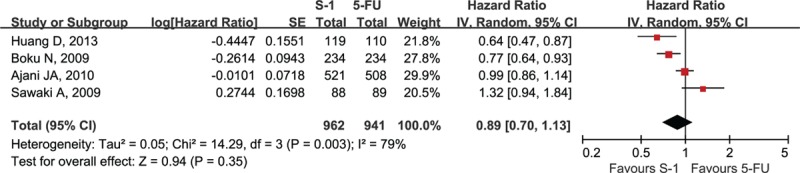
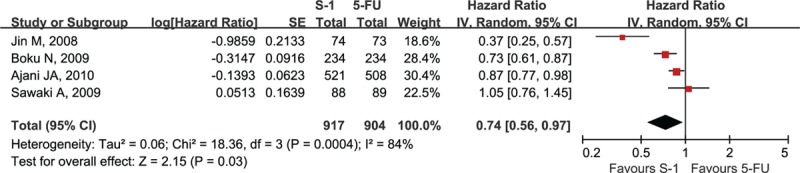
It remains to be seen whether S-1 can be a replacement for infusional fluorouracil (5-FU) for advanced gastric cancer (AGC). The aim of this study was to compare the efficacy and safety of S-1 with 5-FU in AGC.PubMed and Cochrane Library were searched. Randomized controlled trials and meta-analyses comparing S-1 with 5-FU for AGC were eligible. Meta-analysis was performed using RevMan 5.2.Seven trials involving 2443 patients were included. Compared with 5-FU, S-1 showed no significant prolongation of overall survival (OS) (hazard ratio [HR] = 0.91, 95% confidence interval [CI] [0.83-1.01], P = 0.07) and progression-free survival (HR = 0.89, 95% CI [0.70-1.13], P = 0.35), but longer time to treatment failure (HR = 0.74, 95% CI [0.56-0.97], P = 0.03). The objective response rates were comparable (risk ratio [RR] = 1.36, 95% CI [0.95, 1.96], P = 0.10). Regarding treatment-related deaths and hematological toxicities, there was significant heterogeneity between Asian and non-Asian trials, and subgroup analysis was applied. In Asian patients, there was a significant increase in hematological toxicities such as leukopenia (grade 1-4: RR = 1.22, 95% CI [1.08, 1.37], P = 0.001; grade 3-4: RR = 2.21, 95% CI [1.52, 3.21], P < 0.0001), neutropenia (grade 1-4: RR = 1.29, 95% CI [1.11, 1.48], P = 0.0005; grade 3-4: RR = 1.87, 95% CI [1.11, 3.17], P = 0.02), and thrombocytopenia (grade 1-4: RR = 1.71, 95% CI [1.22, 2.41], P = 0.002) in S-1-containing regimens compared with 5-FU-containing regimens, but without significant difference in treatment-related mortality rate (risk difference [RD] = 0.00, 95% CI [-0.01, 0.01], P = 0.68). In non-Asian patients, S-1-containing regimens were, however, associated with significantly fewer treatment-related deaths (RD = -0.02, 95% CI [-0.05, -0.00], P = 0.04), as well as less all grade 1-4 and grade 3-4 hematological toxicities except anemia. There was no significant heterogeneity in nonhematologic toxicities between Asian and non-Asian trials. Lower incidence of grade 1-4 nausea, diarrhea, mucositis, grade 3-4 mucositis, increased creatinine, and decreased calculated creatinine clearance was observed in S-1-containing regimens.S-1 could not improve OS, but increase some hematological toxicities in Asian patients. Therefore, special attention on hematological toxicities should be paid to Asian patients because S-1 is administered on an outpatient basis.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet]. Lyon, France: International Agency for Research on Cancer; Available at: http://globocan.iarc.fr/Pages/fact_sheets_population.aspx Accessed January 17, 2016.
-
- Wagner AD, Grothe W, Haerting J, et al. Chemotherapy in advanced gastric cancer: a systematic review and meta-analysis based on aggregate data. J Clin Oncol 2006;24:2903–9. - PubMed
-
- Wöhrer SS, Raderer M, Hejna M. Palliative chemotherapy for advanced gastric cancer. Ann Oncol 2004;15:1585–95. - PubMed
-
- Boku N. JCOG trials of systemic chemotherapy for unresectable or recurrent gastric cancer. Gastric Cancer 2009;12:43–9.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
