

Indication for Lower Extremity Revascularization and Hospital Profiling of Readmissions
- PMID: 27311949
- PMCID: PMC5894332
- DOI: 10.1016/j.avsg.2016.01.054
Indication for Lower Extremity Revascularization and Hospital Profiling of Readmissions
Abstract
Background: Surgical readmissions are common, costly, and the focus of national quality improvement efforts. Given the relatively high readmission rates among vascular patients, pay-for-performance initiatives such as Medicare's Hospital Readmissions Reduction Program (HRRP) have targeted vascular surgery for increased scrutiny in the near future. Yet, the extent to which institutional case mix influences hospital profiling remains unexplored. We sought to evaluate whether higher readmission rates in vascular surgery are a reflection of worse performance or of treating sicker patients.
Methods: This retrospective observational cohort study of the national Medicare population includes 479,047 beneficiaries undergoing lower extremity revascularization (LER) in 1,701 hospitals from 2005 to 2009. We employed hierarchical logistic regression to mimic Center for Medicare and Medicaid Services methodology accounting for age, gender, preexisting comorbidities, and differences in hospital operative volume. We estimated 30-day risk-standardized readmission rates (RSRR) for each hospital when including (1) all LER patients; (2) claudicants; or (3) high-risk patients (rest pain, ulceration, or tissue loss). We stratified hospitals into quintiles based on overall RSRR for all LERs and examined differences in RSRR for claudicants and high-risk patients between and within quintiles. Next, we evaluated differences in case mix (the proportion of claudicants and high-risk patients treated) across quintiles. Finally, we simulated differences in the receipt of penalties before and after adjusting for hospital case mix.
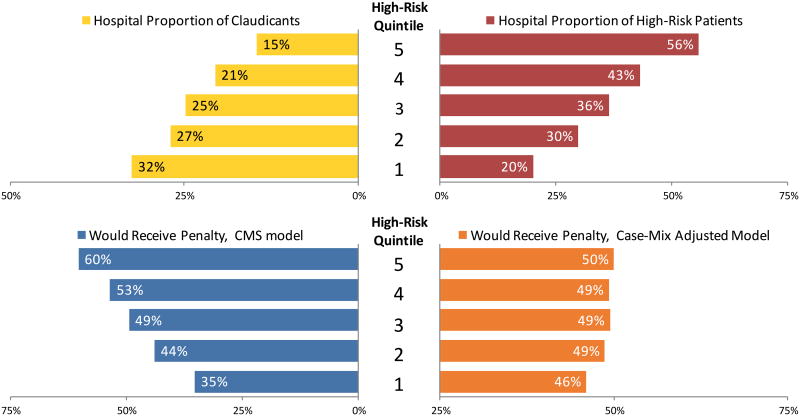
Results: Readmission rates varied widely by indication: 7.3% (claudicants) vs. 19.5% (high risk). Even after adjusting for patient demographics, length of stay, and discharge destination, high-risk patients were significantly more likely to be readmitted (odds ratio 1.76, 95% confidence interval 1.71-1.81). The Best hospitals (top quintile) under the HRRP treated a much lower proportion of high-risk patients compared with the Worst hospitals (bottom quintile) (20% vs. 56%, P < 0.001). In the absence of case-mix adjustment, we observed a stepwise increase in the proportion of hospitals penalized as the proportion of high-risk patients treated increased (35-60%, P < 0.001). However, after case-mix adjustment, there were no differences between quintiles in the proportion of hospitalized penalized (50-46%, P = 0.30).
Conclusion: Our findings suggest that the differences in readmission rates following LER are largely driven by hospital case mix rather than true differences in quality.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Readmission rates after lower extremity bypass vary significantly by surgical indication.J Vasc Surg. 2016 Aug;64(2):458-464. doi: 10.1016/j.jvs.2016.03.422. Epub 2016 Apr 29. J Vasc Surg. 2016. PMID: 27139788
-
Short- and long-term readmission rates after infrainguinal bypass in a safety net hospital are higher than expected.J Vasc Surg. 2017 Dec;66(6):1786-1791. doi: 10.1016/j.jvs.2017.07.120. Epub 2017 Sep 29. J Vasc Surg. 2017. PMID: 28965800
-
Risk factors for readmission after lower extremity procedures for peripheral artery disease.J Vasc Surg. 2013 Jul;58(1):90-7.e1-4. doi: 10.1016/j.jvs.2012.12.031. Epub 2013 Mar 29. J Vasc Surg. 2013. PMID: 23541547
-
A systematic review and meta-analysis of risk factors for and incidence of 30-day readmission after revascularization for peripheral artery disease.J Vasc Surg. 2019 Sep;70(3):996-1006.e7. doi: 10.1016/j.jvs.2019.01.079. J Vasc Surg. 2019. PMID: 31445653
-
The Hospital Readmissions Reduction Program: Nationwide Perspectives and Recommendations: A JACC: Heart Failure Position Paper.JACC Heart Fail. 2020 Jan;8(1):1-11. doi: 10.1016/j.jchf.2019.07.012. Epub 2019 Oct 9. JACC Heart Fail. 2020. PMID: 31606360 Review.
Cited by
-
Association between readmission care fragmentation and outcomes after interventions for peripheral arterial disease.J Vasc Surg. 2023 Dec;78(6):1513-1522.e1. doi: 10.1016/j.jvs.2023.08.125. Epub 2023 Aug 30. J Vasc Surg. 2023. PMID: 37657686 Free PMC article.
-
Daly/Cost comparison in the management of peripheral arterial disease at 17 Belgian hospitals.BMC Health Serv Res. 2024 Jan 19;24(1):109. doi: 10.1186/s12913-023-10535-2. BMC Health Serv Res. 2024. PMID: 38243251 Free PMC article.
-
Factors associated with 90-day reintervention following lower extremity revascularization.J Vasc Surg. 2024 Jul;80(1):213-222.e1. doi: 10.1016/j.jvs.2024.03.009. Epub 2024 Mar 8. J Vasc Surg. 2024. PMID: 38462063 Free PMC article.
-
Prescriptive analytics for reducing 30-day hospital readmissions after general surgery.PLoS One. 2020 Sep 9;15(9):e0238118. doi: 10.1371/journal.pone.0238118. eCollection 2020. PLoS One. 2020. PMID: 32903282 Free PMC article.
-
How Do We Prevent Readmissions After Major Surgery?Adv Surg. 2017 Sep;51(1):89-100. doi: 10.1016/j.yasu.2017.03.007. Epub 2017 May 13. Adv Surg. 2017. PMID: 28797348 Free PMC article. Review. No abstract available.
References
-
- Centers for Medicare & Medicaid Services. Readmissions Reduction Program [Internet] 2012 Available from: http://go.cms.gov/1eUTfaO.
-
- Suter LG, Grady JN, Lin Z, Parzynski CS, Potteiger J, Keenan M, et al. 2013 Measure Updates and Specifications : Elective Primary Total Hip Arthroplasty (THA) And / Or Total Knee Arthroplasty (TKA) All-Cause Unplanned 30-Day Risk-Standardized Readmission Measure [Internet] New Haven. 2013 Available from: http://bit.ly/Pnuj2o.
-
- Medicare Payment Advisory Commission (MedPAC) Report to Congress: Promoting Greater Efficiency in Medicare [Internet] 2007;Chapter 5 Available from: http://1.usa.gov/1lp2gJ9.
-
- Bosco JLF, Silliman Ra, Thwin SS, Geiger AM, Buist DSM, Prout MN, et al. J Clin Epidemiol [Internet] 1. Vol. 63. Elsevier Inc; 2010. A most stubborn bias: no adjustment method fully resolves confounding by indication in observational studies; pp. 64–74. Available from: http://dx.doi.org/10.1016/j.jclinepi.2009.03.001. - DOI - PMC - PubMed
-
- McPhee JT, Barshes NR, Ho KJ, Madenci A, Ozaki CK, Nguyen LL, et al. Predictive factors of 30-day unplanned readmission after lower extremity bypass. J Vasc Surg. 2013 Apr;57(4):955–62. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
