

Healthcare Burden, Risk Factors, and Outcomes of Mucosal Barrier Injury Laboratory-Confirmed Bloodstream Infections after Stem Cell Transplantation
- PMID: 27311966
- PMCID: PMC5685512
- DOI: 10.1016/j.bbmt.2016.06.002
Healthcare Burden, Risk Factors, and Outcomes of Mucosal Barrier Injury Laboratory-Confirmed Bloodstream Infections after Stem Cell Transplantation
Abstract
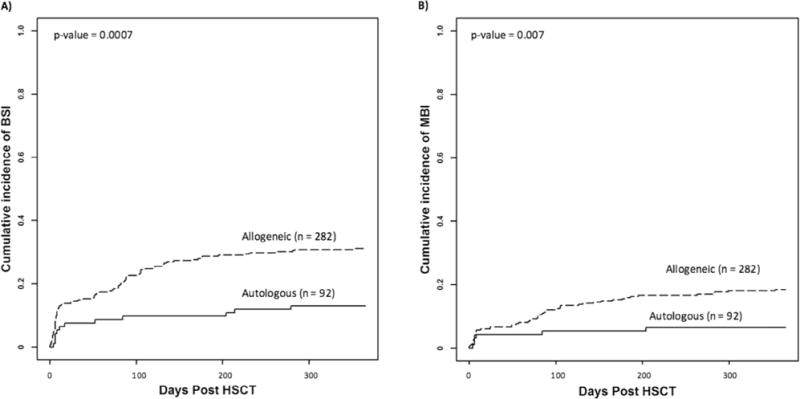
Mucosal barrier injury laboratory-confirmed bloodstream infections (MBI-LCBIs) lead to significant morbidity, mortality, and healthcare resource utilization in hematopoietic stem cell transplant (HSCT) patients. Determination of the healthcare burden of MBI-LCBIs and identification of patients at risk of MBI-LCBIs will allow researchers to identify strategies to reduce MBI-LCBI rates. The objective of our study was to describe the incidence, risk factors, timing, and outcomes of MBI-LCBIs in hematopoietic stem cell transplant patients. We performed a retrospective analysis of 374 patients who underwent HSCT at a large free-standing academic children's hospital to determine the incidence, risk factors, and outcomes of patients that developed a bloodstream infection (BSI) including MBI-LCBI, central line-associated BSI (CLABSI), or secondary BSI in the first year after HSCT. Outcome measures included nonrelapse mortality (NRM), central venous catheter removal within 7 days of positive culture, shock, admission to the pediatric intensive care unit (PICU) within 48 hours of positive culture, and death within 10 days of positive culture. One hundred seventy BSIs were diagnosed in 100 patients (27%): 80 (47%) MBI-LCBIs, 68 (40%) CLABSIs, and 22 (13%) secondary infections. MBI-LCBIs were diagnosed at a significantly higher rate in allogeneic HSCT patients (18% versus 7%, P = .007). Reduced-intensity conditioning (OR, 1.96; P = .015) and transplant-associated thrombotic microangiopathy (OR, 2.94; P = .0004) were associated with MBI-LCBI. Nearly 50% of all patients with a BSI developed septic shock, 10% died within 10 days of positive culture, and nearly 25% were transferred to the PICU. One-year NRM was significantly increased in patients with 1 (34%) and more than 1 (56%) BSIs in the first year post-HSCT compared with those who did not develop BSIs (14%) (P ≤ .0001). There was increased 1-year NRM in patients with at least 1 MBI-LCBI (OR, 1.94; P = .018) and at least 1 secondary BSI (OR, 2.87; P = .0023) but not CLABSIs (OR, 1.17; P = .68). Our data demonstrate that MBI-LCBIs lead to substantial use of healthcare resources and are associated with significant morbidity and mortality. Reduction in frequency of MBI-LCBI should be a major public health and scientific priority.
Keywords: Bloodstream infection; CLABSI; Central line–associated bloodstream infection; Hematopoietic stem cell transplantation; MBI-LCBI; Mucosal barrier injury laboratory-confirmed bloodstream infection; Transplant-associated thrombotic microangiopathy.
Copyright © 2016 The American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures

References
-
- Poutsiaka DD, Price LL, Ucuzian A, Chan GW, Miller KB, Snydman DR. Blood stream infection after hematopoietic stem cell transplantation is associated with increased mortality. Bone Marrow Transplant. 2007;40:63–70. - PubMed
-
- See I, Iwamoto M, Allen-Bridson K, Horan T, Magill SS, Thompson ND. Mucosal barrier injury laboratory-confirmed bloodstream infection: results from a field test of a new National Healthcare Safety Network definition. Infect Control Hosp Epidemiol. 2013;34:769–776. - PubMed
-
- Wilson MZ, Rafferty C, Deeter D, Comito MA, Hollenbeak CS. Attributable costs of central line-associated bloodstream infections in a pediatric hematology/oncology population. Am J Infect Control. 2014;42:1157–1160. - PubMed
-
- Cecinati V, Brescia L, Tagliaferri L, Giordano P, Esposito S. Catheter-related infections in pediatric patients with cancer. Eur J Clin Microbiol Infect Dis. 2012;31:2869–2877. - PubMed
-
- Bundy DG, Gaur AH, Billett AL, et al. Preventing CLABSIs among pediatric hematology/oncology inpatients: national collaborative results. Pediatrics. 2014;134:e1678–e1685. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
