

Systematic Evaluation of the Cellular Innate Immune Response During the Process of Human Atherosclerosis
- PMID: 27312803
- PMCID: PMC4937250
- DOI: 10.1161/JAHA.115.002860
Systematic Evaluation of the Cellular Innate Immune Response During the Process of Human Atherosclerosis
Abstract
Background: The concept of innate immunity is well recognized within the spectrum of atherosclerosis, which is primarily dictated by macrophages. Although current insights to this process are largely based on murine models, there are fundamental differences in the atherosclerotic microenvironment and associated inflammatory response relative to humans. In this light, we characterized the cellular aspects of innate immune response in normal, nonprogressive, and progressive human atherosclerotic plaques.
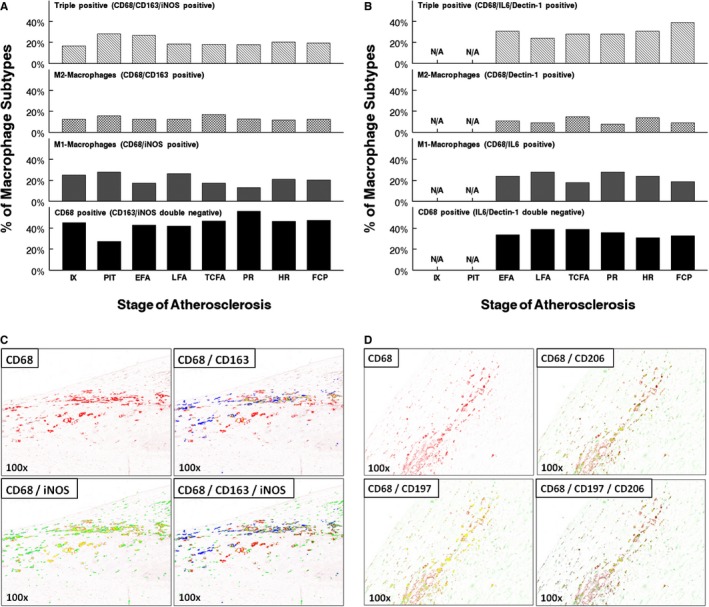
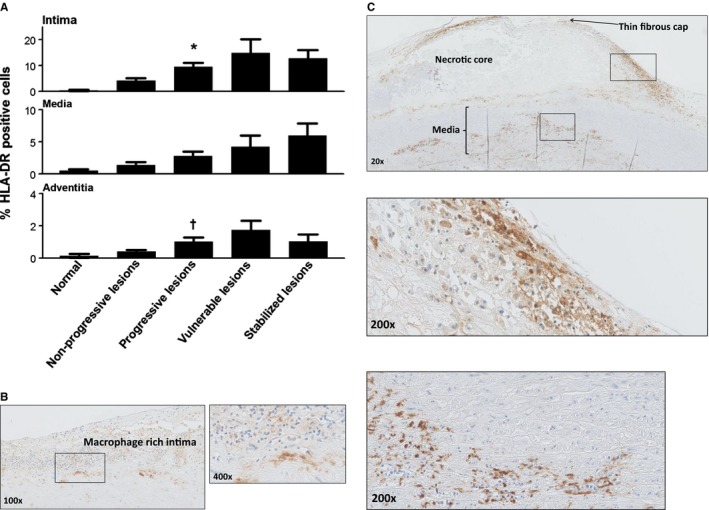
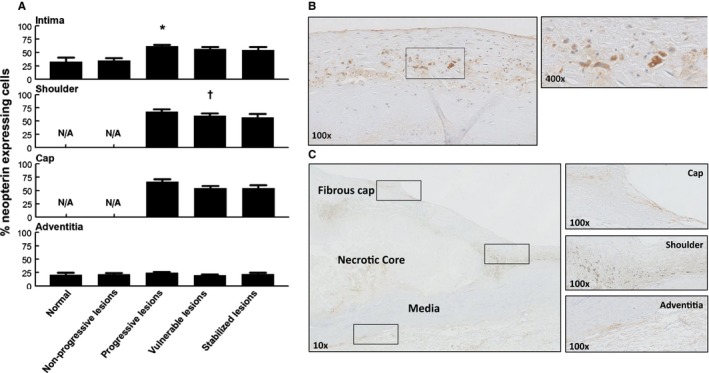
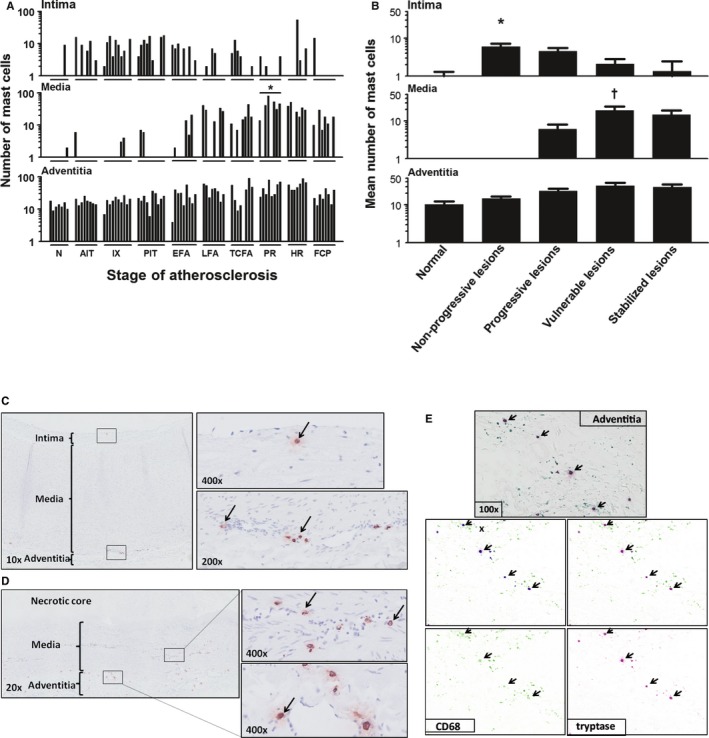
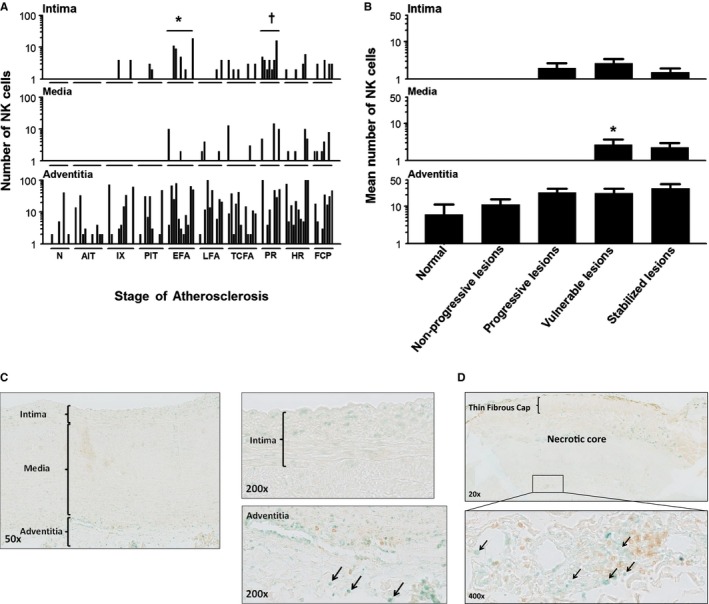
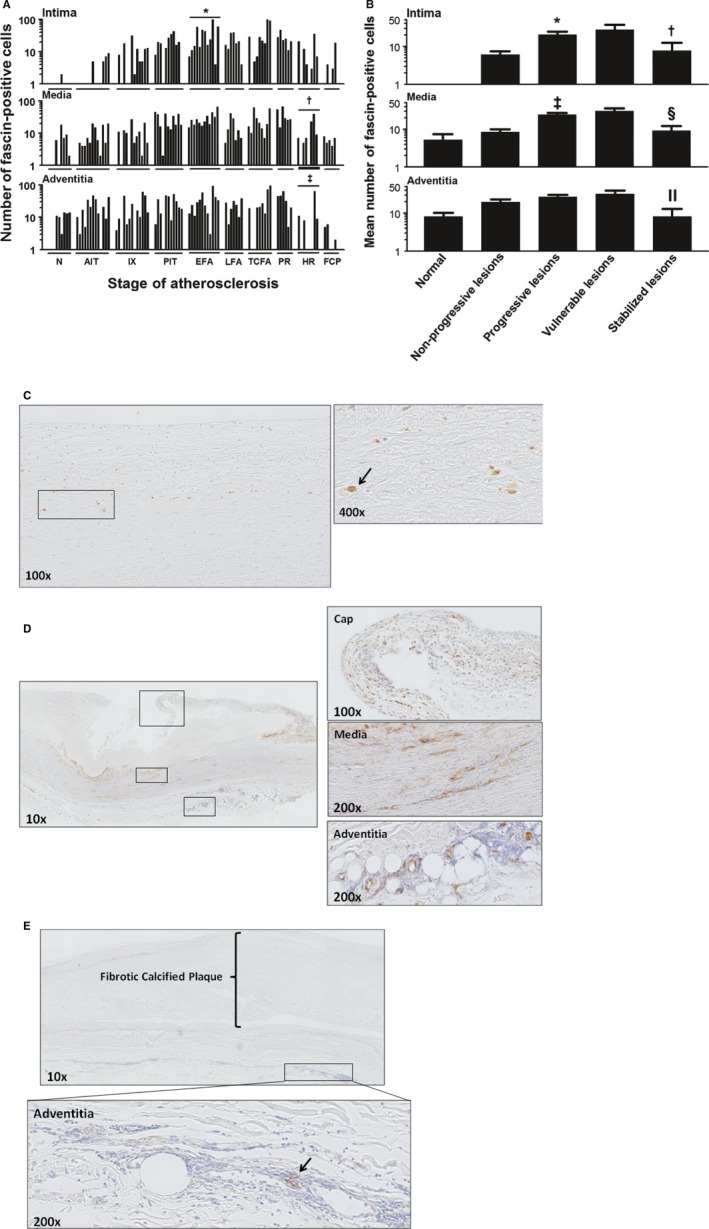
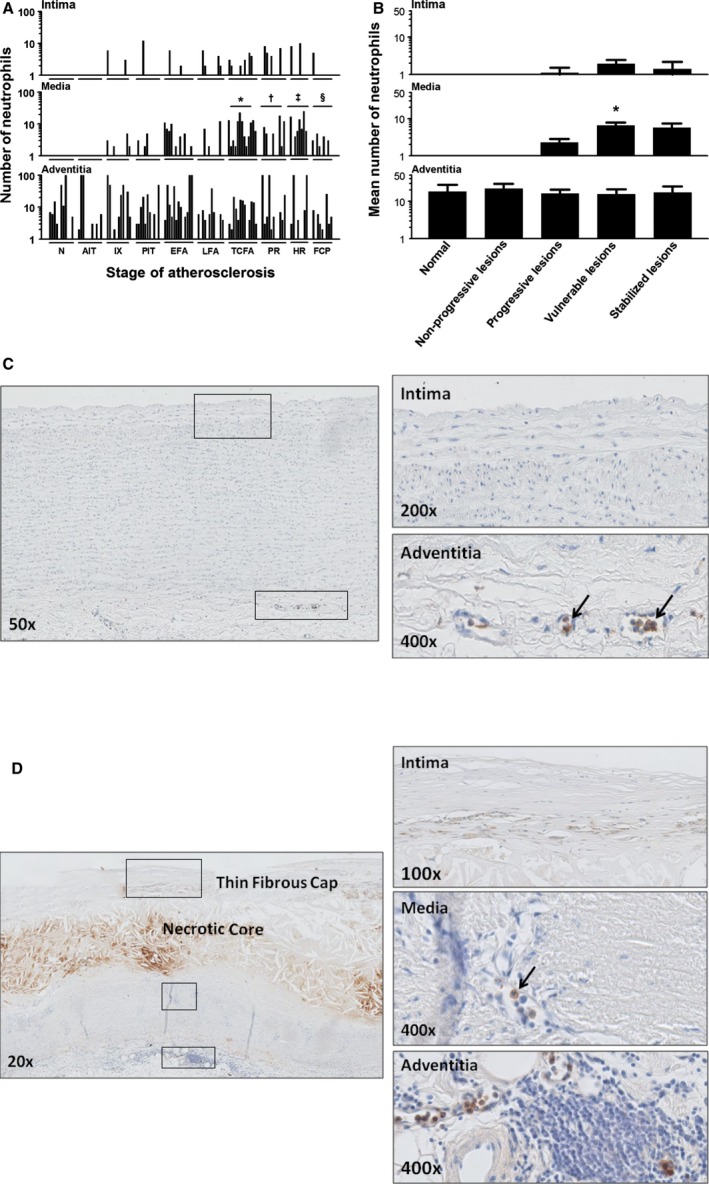
Methods and results: A systematic analysis of innate immune response was performed on 110 well-characterized human perirenal aortic plaques with immunostaining for specific macrophage subtypes (M1 and M2 lineage) and their activation markers, neopterin and human leukocyte antigen-antigen D related (HLA-DR), together with dendritic cells (DCs), natural killer (NK) cells, mast cells, neutrophils, and eosinophils. Normal aortae were devoid of low-density lipoprotein, macrophages, DCs, NK cells, mast cells, eosinophils, and neutrophils. Early, atherosclerotic lesions exhibited heterogeneous populations of (CD68(+)) macrophages, whereby 25% were double positive "M1" (CD68(+)/ inducible nitric oxide synthase [iNOS](+)/CD163(-)), 13% "M2" double positive (CD68(+)/iNOS(-)/CD163(+)), and 17% triple positive for (M1) iNOS (M2)/CD163 and CD68, with the remaining (≈40%) only stained for CD68. Progressive fibroatheromatous lesions, including vulnerable plaques, showed increasing numbers of NK cells and fascin-positive cells mainly localized to the media and adventitia whereas the M1/M2 ratio and level of macrophage activation (HLA-DR and neopterin) remained unchanged. On the contrary, stabilized (fibrotic) plaques showed a marked reduction in macrophages and cell activation with a concomitant decrease in NK cells, DCs, and neutrophils.
Conclusions: Macrophage "M1" and "M2" subsets, together with fascin-positive DCs, are strongly associated with progressive and vulnerable atherosclerotic disease of human aorta. The observations here support a more complex theory of macrophage heterogeneity than the existing paradigm predicated on murine data and further indicate the involvement of (poorly defined) macrophage subtypes or greater dynamic range of macrophage plasticity than previously considered.
Keywords: aorta; atherosclerosis; immune system; inflammation; macrophage.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Fernández‐Velasco M, González‐Ramos S, Boscá L. Involvement of monocytes/macrophages as key factors in the development and progression of cardiovascular diseases. Biochem J. 2014;458:187–193. - PubMed
-
- Hansson GK, Libby P, Schönbeck U, Yan ZQ. Innate and adaptive immunity in the pathogenesis of atherosclerosis. Circ Res. 2002;91:281–291. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
