

Obstructive Sleep Apnea: A Cluster Analysis at Time of Diagnosis
- PMID: 27314230
- PMCID: PMC4912165
- DOI: 10.1371/journal.pone.0157318
Obstructive Sleep Apnea: A Cluster Analysis at Time of Diagnosis
Abstract
Background: The classification of obstructive sleep apnea is on the basis of sleep study criteria that may not adequately capture disease heterogeneity. Improved phenotyping may improve prognosis prediction and help select therapeutic strategies.
Objectives: This study used cluster analysis to investigate the clinical clusters of obstructive sleep apnea.
Methods: An ascending hierarchical cluster analysis was performed on baseline symptoms, physical examination, risk factor exposure and co-morbidities from 18,263 participants in the OSFP (French national registry of sleep apnea). The probability for criteria to be associated with a given cluster was assessed using odds ratios, determined by univariate logistic regression.
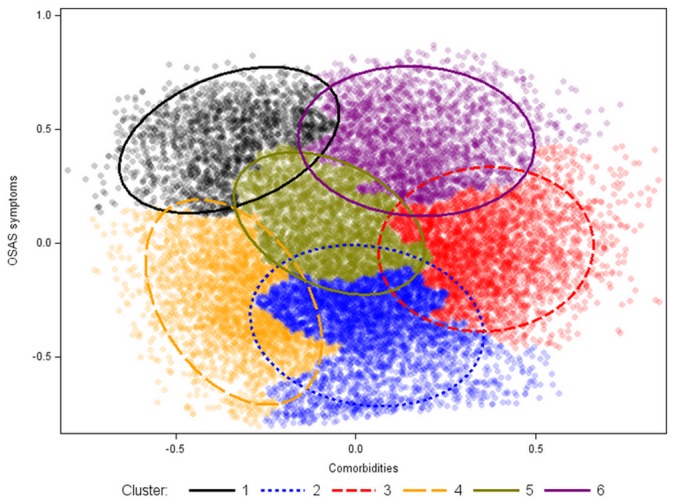
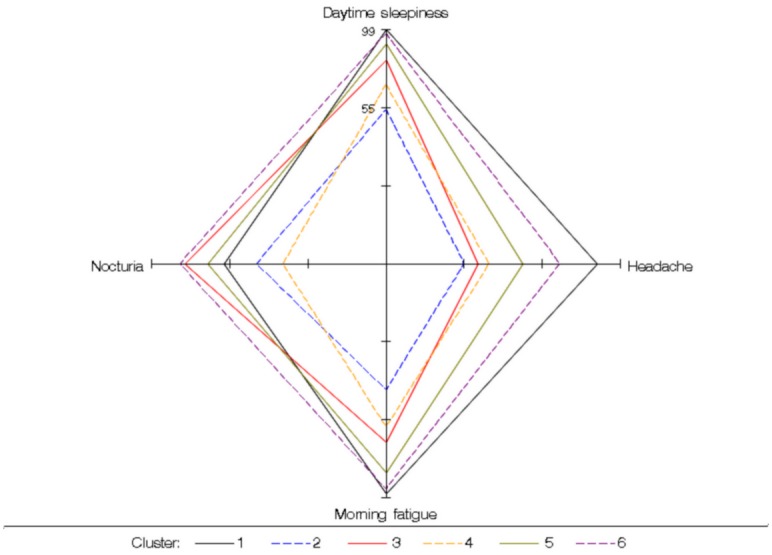
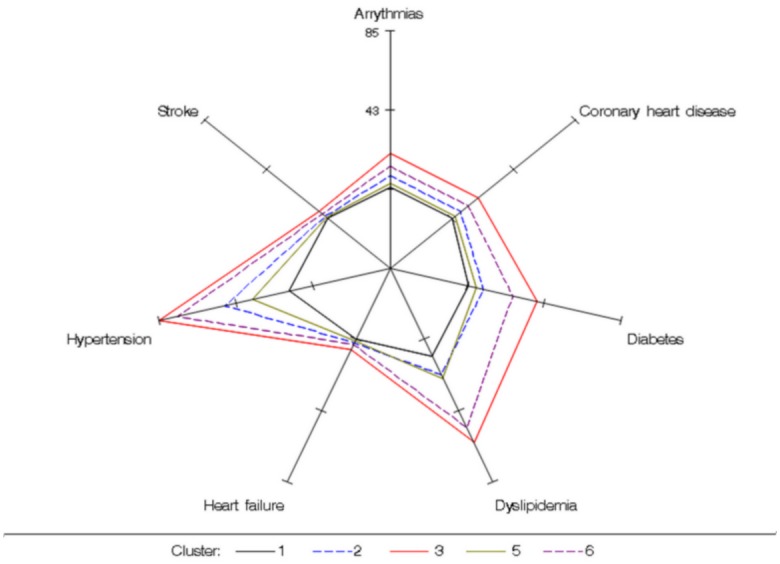
Results: Six clusters were identified, in which patients varied considerably in age, sex, symptoms, obesity, co-morbidities and environmental risk factors. The main significant differences between clusters were minimally symptomatic versus sleepy obstructive sleep apnea patients, lean versus obese, and among obese patients different combinations of co-morbidities and environmental risk factors.
Conclusions: Our cluster analysis identified six distinct clusters of obstructive sleep apnea. Our findings underscore the high degree of heterogeneity that exists within obstructive sleep apnea patients regarding clinical presentation, risk factors and consequences. This may help in both research and clinical practice for validating new prevention programs, in diagnosis and in decisions regarding therapeutic strategies.
Conflict of interest statement
Figures

References
-
- Berry RB, Budhiraja R, Gottlieb DJ, Gozal D, Iber C, Kapur VK, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2012;8(5):597–619. Epub 2012/10/16. 10.5664/jcsm.2172 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
