

Defining the optimal sequence for the systemic treatment of metastatic breast cancer
- PMID: 27314861
- PMCID: PMC5239809
- DOI: 10.1007/s12094-016-1520-2
Defining the optimal sequence for the systemic treatment of metastatic breast cancer
Abstract
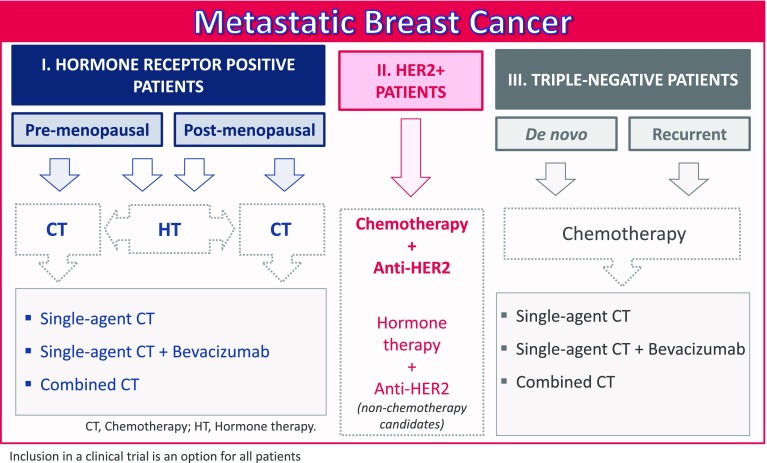
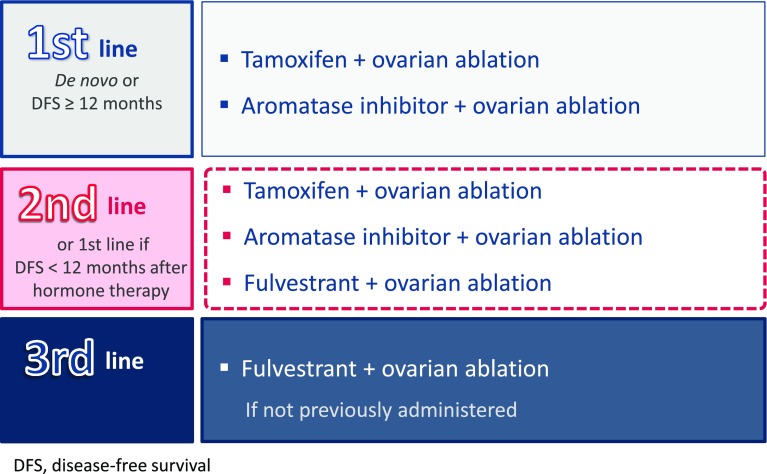
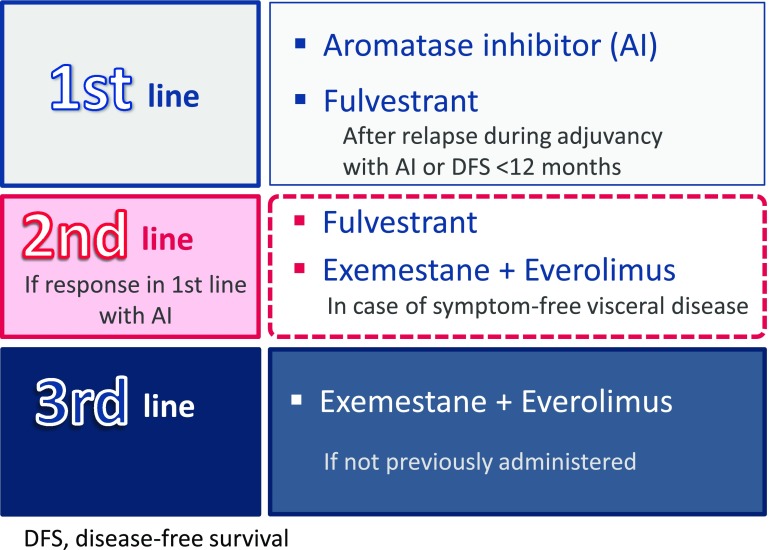
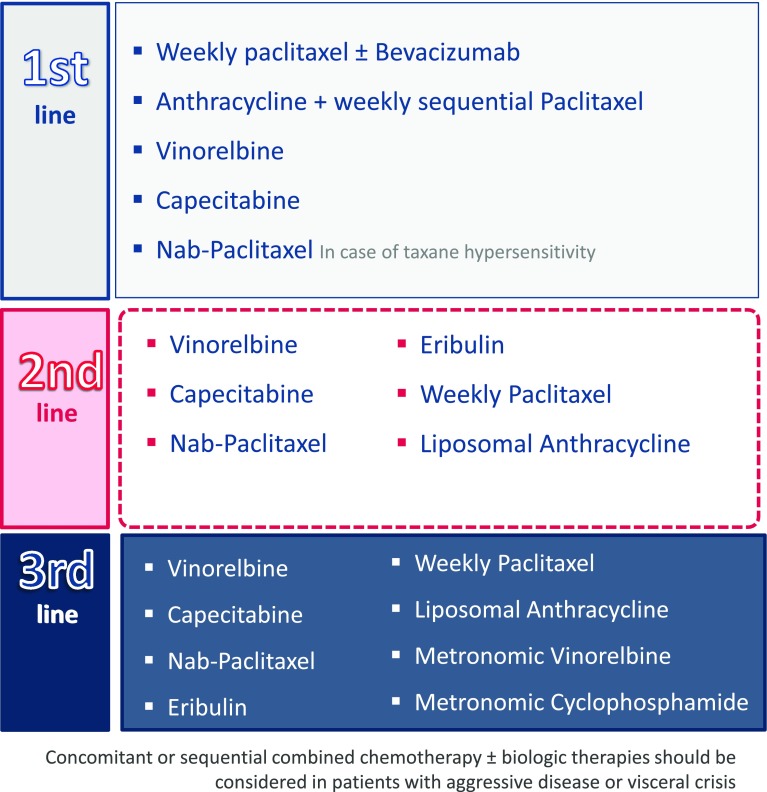
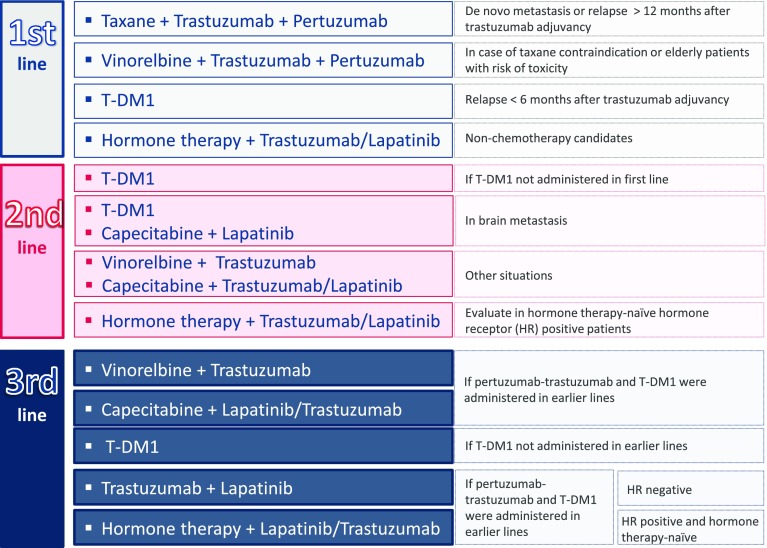
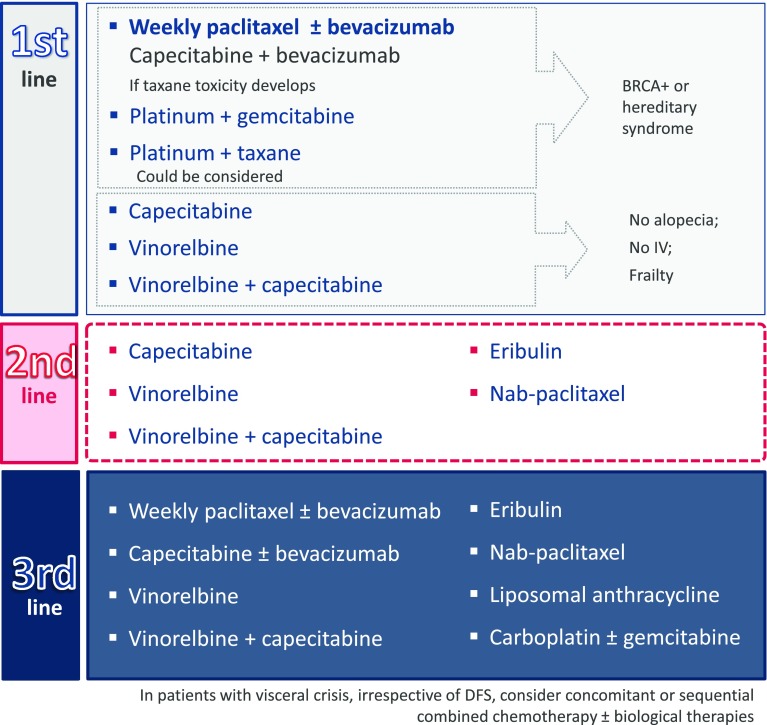
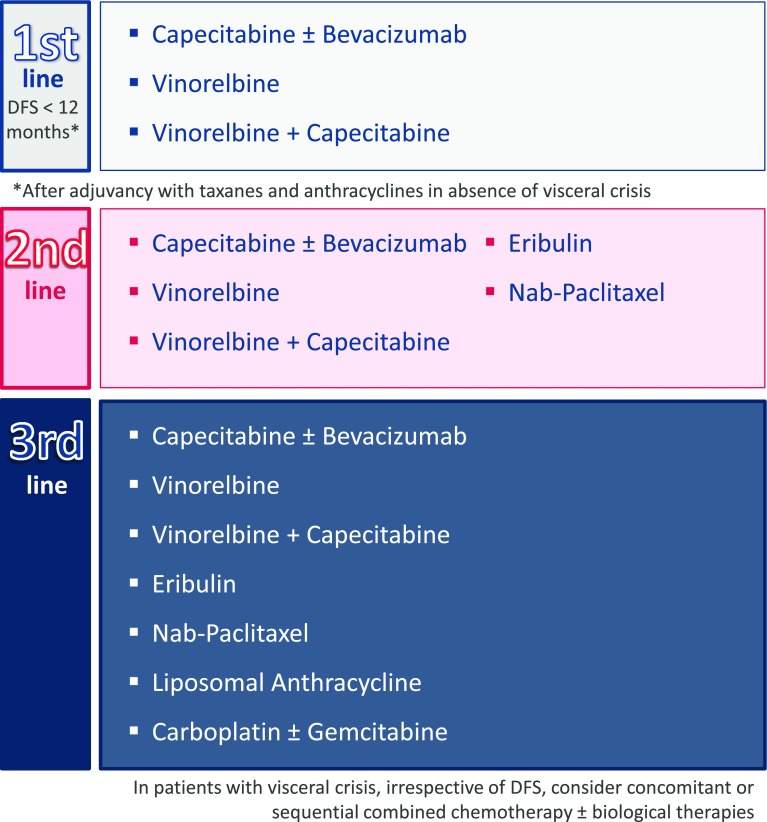
Metastatic breast cancer is a heterogeneous disease that presents in varying forms, and a growing number of therapeutic options makes it difficult to determine the best choice in each particular situation. When selecting a systemic treatment, it is important to consider the medication administered in the previous stages, such as acquired resistance, type of progression, time to relapse, tumor aggressiveness, age, comorbidities, pre- and post-menopausal status, and patient preferences. Moreover, tumor genomic signatures can identify different subtypes, which can be used to create patient profiles and design specific therapies. However, there is no consensus regarding the best treatment sequence for each subgroup of patients. During the SABCC Congress of 2014, specialized breast cancer oncologists from referral hospitals in Europe met to define patient profiles and to determine specific treatment sequences for each one. Conclusions were then debated in a final meeting in which a relative degree of consensus for each treatment sequence was established. Four patient profiles were defined according to established breast cancer phenotypes: pre-menopausal patients with luminal subtype, post-menopausal patients with luminal subtype, patients with triple-negative subtype, and patients with HER2-positive subtype. A treatment sequence was then defined, consisting of hormonal therapy with tamoxifen, aromatase inhibitors, fulvestrant, and mTOR inhibitors for pre- and post-menopausal patien ts; a chemotherapy sequence for the first, second, and further lines for luminal and triple-negative patients; and an optimal sequence for treatment with new antiHER2 therapies. Finally, a document detailing all treatment sequences, that had the agreement of all the oncologists, was drawn up as a guideline and advocacy tool for professionals treating patients with this disease.
Keywords: Chemotherapy; HER2 receptor; Hormone therapy; Metastatic breast cancer; Targeted therapies; Triple-negative tumor.
Conflict of interest statement
The authors declare no conflict of interest. Research involving human participants and/or animals Not applicable to this type of consensus document. Informed consent Not applicable to this type of consensus document.
Figures
References
-
- Sanchez MJ, Payer T, De Angelis R, Larranaga N, Capocaccia R, Martinez C. Cancer incidence and mortality in Spain: estimates and projections for the period 1981–2012. Ann Oncol. 2010;21(3):iii30–iii36. - PubMed
-
- Puig-Vives M, Sanchez MJ, Sanchez-Cantalejo J, Torrella-Ramos A, Martos C, Ardanaz E, et al. Distribution and prognosis of molecular breast cancer subtypes defined by immunohistochemical biomarkers in a Spanish population-based study. Gynecol Oncol. 2013;130(3):609–614. doi: 10.1016/j.ygyno.2013.05.039. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
