

Association of Vasomotor and Other Menopausal Symptoms with Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis
- PMID: 27315068
- PMCID: PMC4912069
- DOI: 10.1371/journal.pone.0157417
Association of Vasomotor and Other Menopausal Symptoms with Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis
Abstract
Importance: Vasomotor symptoms (hot flushes and night sweats) and other symptoms, including depression, anxiety and panic attacks, are commonly experienced by menopausal women and have been associated with an unfavourable cardiovascular risk profile.
Objective: To investigate whether presence of menopausal symptoms is associated with the development of cardiovascular disease (CVD).
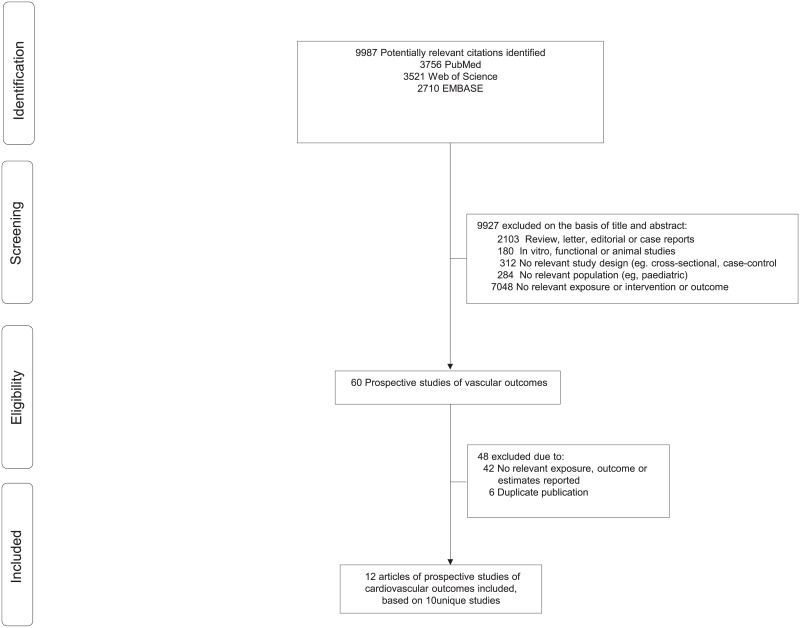
Methods: Five electronic databases (Medline, EMBASE and Web of Science) were search until February 17th, 2015 to identify relevant studies. Observational cohort studies or randomised intervention studies were eligible for inclusion if they followed participants prospectively (at least 1 year of follow-up), and reported relevant estimates on the association of any vasomotor symptoms, or other menopausal symptoms, with risk of CVD, coronary heart disease (CHD), or stroke in perimenopausal, menopausal, or postmenopausal women. Data were extracted by two independent reviewers using a pre-designed data collection form. Separate pooled relative risks (RRs) for age and non-established cardiovascular risk factors (e.g., education, ethnicity) adjusted data and for established cardiovascular risk factors and potential mediators-adjusted data (e.g., smoking, body mass index, and hypertension) were calculated.
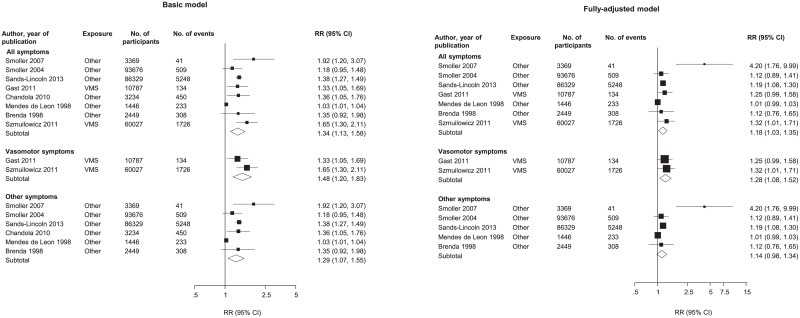
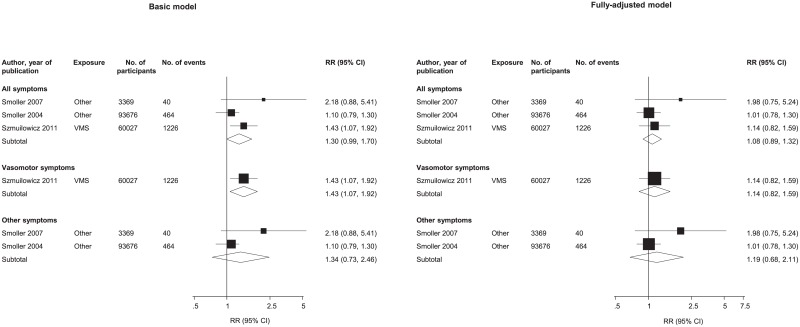
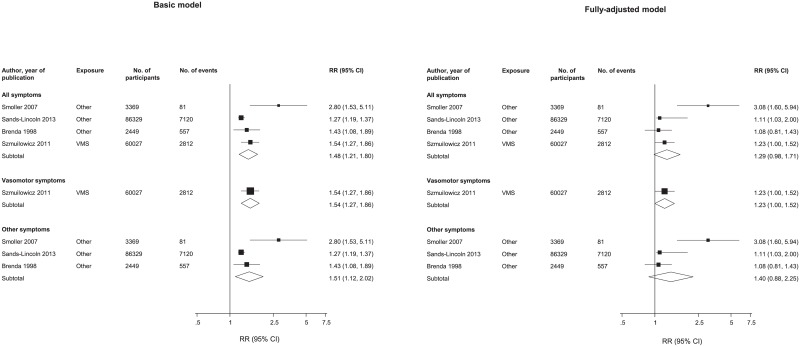
Results: Out of 9,987 initially identified references, ten studies were selected, including 213,976 women with a total of 10,037 cardiovascular disease outcomes. The age and non-established cardiovascular risk factors adjusted RRs) [95% confidence intervals] for development of CHD, Stroke and CVD comparing women with and without any menopausal symptoms were 1.34 [1.13-1.58], 1.30 [0.99-1.70], 1.48 [1.21-1.80] respectively, and the corresponding RRs adjusted for cardiovascular risk factors and potential mediators were 1.18 [1.03-1.35], 1.08 [0.89-1.32], 1.29 [0.98-1.71]. However, these analyses were limited by potential unmeasured confounding and the small number of studies on this topic.
Conclusion: Presence of vasomotor symptoms and other menopausal symptoms are generally associated with an increased risk of cardiovascular disease, which is mainly explained by cardiovascular risk factors.
Conflict of interest statement
Figures
Similar articles
-
Long-term hormone therapy for perimenopausal and postmenopausal women.Cochrane Database Syst Rev. 2017 Jan 17;1(1):CD004143. doi: 10.1002/14651858.CD004143.pub5. Cochrane Database Syst Rev. 2017. PMID: 28093732 Free PMC article.
-
Exercise for vasomotor menopausal symptoms.Cochrane Database Syst Rev. 2007 Oct 17;(4):CD006108. doi: 10.1002/14651858.CD006108.pub2. Cochrane Database Syst Rev. 2007. Update in: Cochrane Database Syst Rev. 2011 May 11;(5):CD006108. doi: 10.1002/14651858.CD006108.pub3. PMID: 17943886 Updated.
-
Exercise for vasomotor menopausal symptoms.Cochrane Database Syst Rev. 2011 May 11;(5):CD006108. doi: 10.1002/14651858.CD006108.pub3. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2014 Nov 28;(11):CD006108. doi: 10.1002/14651858.CD006108.pub4. PMID: 21563149 Updated.
-
Black cohosh (Cimicifuga spp.) for menopausal symptoms.Cochrane Database Syst Rev. 2012 Sep 12;2012(9):CD007244. doi: 10.1002/14651858.CD007244.pub2. Cochrane Database Syst Rev. 2012. PMID: 22972105 Free PMC article.
-
Phytoestrogens for vasomotor menopausal symptoms.Cochrane Database Syst Rev. 2007 Oct 17;(4):CD001395. doi: 10.1002/14651858.CD001395.pub3. Cochrane Database Syst Rev. 2007. Update in: Cochrane Database Syst Rev. 2013 Dec 10;(12):CD001395. doi: 10.1002/14651858.CD001395.pub4. PMID: 17943751 Updated.
Cited by
-
Comparison of urinary adiponectin in the presence of metabolic syndrome in peri- and postmenopausal women.BMC Womens Health. 2022 Mar 14;22(1):70. doi: 10.1186/s12905-022-01655-8. BMC Womens Health. 2022. PMID: 35287667 Free PMC article.
-
Extended afternoon naps are associated with hypertension in women but not in men.Heart Lung. 2020 Jan-Feb;49(1):2-9. doi: 10.1016/j.hrtlng.2019.09.002. Epub 2019 Sep 11. Heart Lung. 2020. PMID: 31521340 Free PMC article.
-
Sex-Specific Physiology and Cardiovascular Disease.Adv Exp Med Biol. 2018;1065:433-454. doi: 10.1007/978-3-319-77932-4_27. Adv Exp Med Biol. 2018. PMID: 30051400 Free PMC article. Review.
-
Benign prostatic hyperplasia is associated with increased 90-day medical complications but not peri-prosthetic joint infections following reverse shoulder arthroplasty.Eur J Orthop Surg Traumatol. 2023 Jul;33(5):1773-1779. doi: 10.1007/s00590-022-03344-6. Epub 2022 Aug 11. Eur J Orthop Surg Traumatol. 2023. PMID: 35951116
-
Cardiovascular Disease Risk in Women with Menopause.J Clin Med. 2025 May 23;14(11):3663. doi: 10.3390/jcm14113663. J Clin Med. 2025. PMID: 40507425 Free PMC article. Review.
References
-
- Dennerstein L, Dudley EC, Hopper JL, Guthrie JR, Burger HG. A prospective population-based study of menopausal symptoms. Obstet Gynecol. 2000;96(3):351–8. Epub 2000/08/29. doi: S0029-7844(00)00930-3 [pii]. . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
