

MRI characteristics of proctitis in Crohn's disease on perianal MRI
- PMID: 27315072
- PMCID: PMC5018025
- DOI: 10.1007/s00261-016-0802-z
MRI characteristics of proctitis in Crohn's disease on perianal MRI
Abstract
Purpose: Multiple features have been described for assessing inflammation in Crohn's disease (CD) in MR enterography, but have not been validated in perianal magnetic resonance imaging (MRI). Retrospectively, we studied which MRI features are valuable in assessing proctitis.
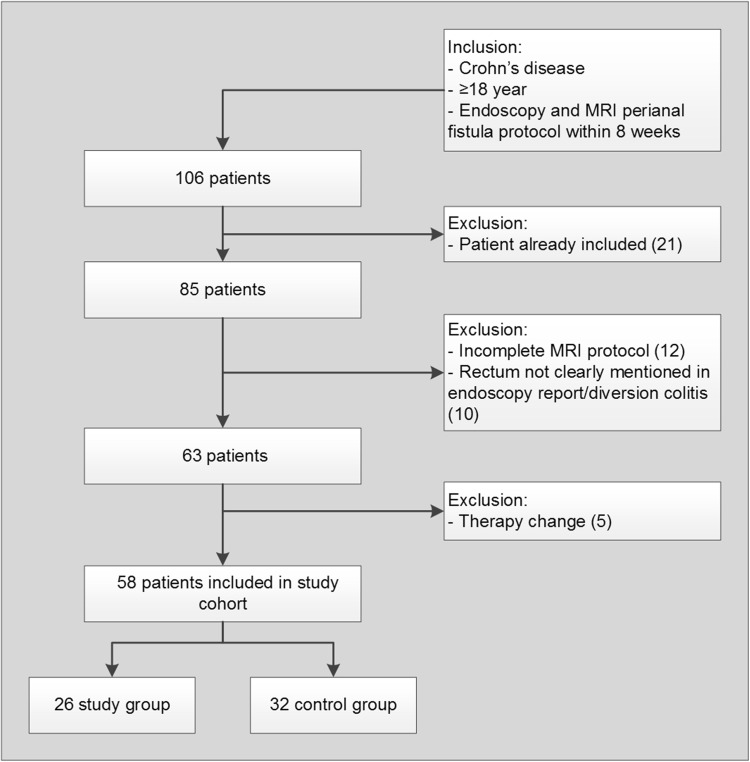
Materials and methods: CD patients (≥18 years) who underwent colonoscopy (reference standard) and perianal fistula MRI within 8 weeks were included. Seventeen MRI features were blindly scored by three observers and correlated to endoscopy (regression analysis). Reproducibility (multirater kappa, intraclass correlation coefficient) was determined for all three observer pairs. MRI features were considered relevant when significantly correlated to endoscopy for ≥2 observers, and reproducibility was ≥0.40 for ≥2 observer pairs.
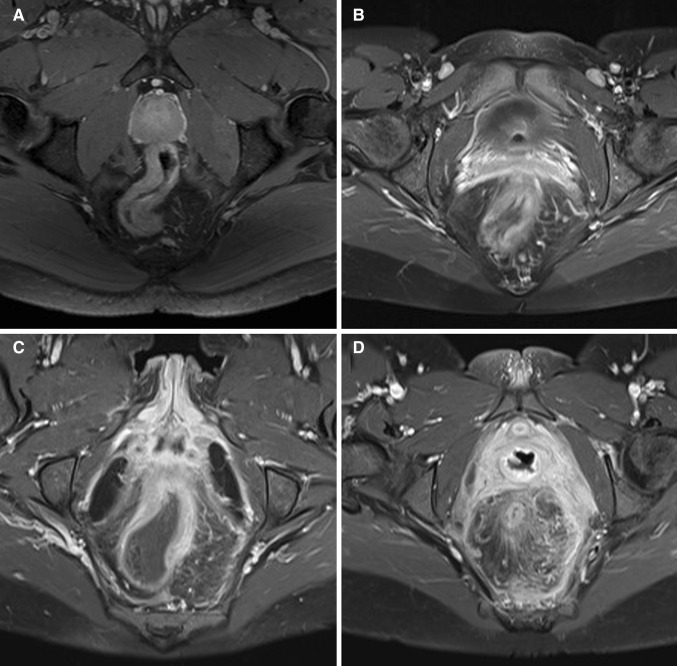
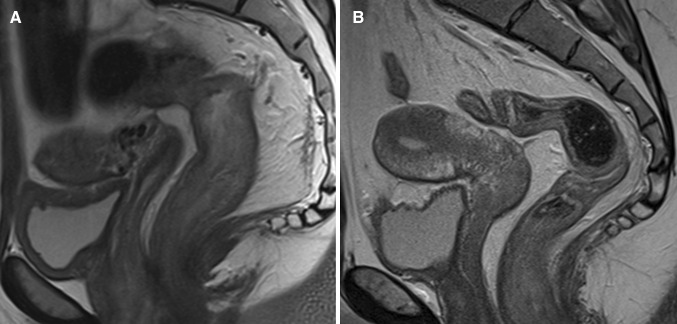
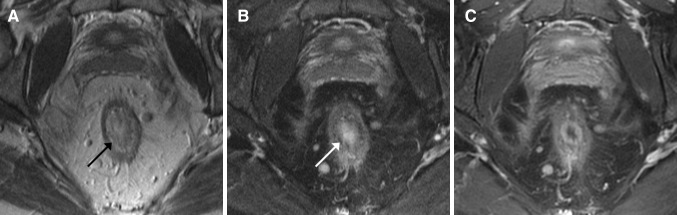
Results: Perianal MRI of 58 CD patients were included. Wall thickness, rectal mural fat, creeping fat, and size of mesorectal lymph nodes showed a significant correlation with endoscopy for ≥2 observers (p = 0.000-0.023, p = 0.011-0.172, p = 0.007-0.011 and p = 0.000-0.005, respectively) with a kappa/intraclass correlation coefficient of ≥0.60 for ≥2 observer pairs. Perimural T2 signal and perimural enhancement significantly correlated to endoscopy (all p values ≤0.05) for all three observers and the reproducibility was ≥0.40 for ≥2 observer pairs. Mural T2 signal and degree and pattern of T1 enhancement showed significant correlation to endoscopy for two observers, but with poor to moderate reproducibility.
Conclusion: Wall thickness, mural fat, and mesorectal features (perimural T2 signal, perimural enhancement, creeping fat, and size of mesorectal lymph nodes) had significant correlation to endoscopy and were reproducible in diagnosing proctitis. Some established luminal features in MRE were considered not useful.
Keywords: Crohn disease; Inflammatory bowel disease; Magnetic resonance imaging; Proctitis; Rectum.
Conflict of interest statement
Compliance with ethical standards Funding This study received no funding. For none of the authors of this manuscript any financial interest is applicable. Disclosures Professor J. Stoker is a consultant for Robarts. Dr.C.Y. Ponsioen has received unconditional grants from Takeda, served as a consultant for Takeda and Abbvie, and received speaker’s fees from Takeda, MSD, Ferring, Dr. Falk, and Abbvie. All other authors, C.J. Tutein Nolthenius, S. Bipat, B. Mearadji, S. Spijkerboer, and A.D. Montauban van Swijndregt, have nothing to disclose. Informed consent The requirement for review by the Medical Ethical Committee or informed consent was waived because of the retrospective nature of this study with pre-existing data.
Figures
Similar articles
-
Evaluation of Crohn's disease activity by MR enterography: Derivation and histopathological comparison of an MR-based activity index.Eur J Radiol. 2015 Oct;84(10):1829-34. doi: 10.1016/j.ejrad.2015.06.005. Epub 2015 Jun 9. Eur J Radiol. 2015. PMID: 26123842
-
Impact of gadolinium-based contrast agent in the assessment of Crohn's disease activity: Is contrast agent injection necessary?J Magn Reson Imaging. 2016 Mar;43(3):688-97. doi: 10.1002/jmri.25024. Epub 2015 Aug 6. J Magn Reson Imaging. 2016. PMID: 26250897
-
Retrospective comparison of magnetic resonance imaging features and histopathology in Crohn's disease patients.Eur J Radiol. 2011 Dec;80(3):e299-305. doi: 10.1016/j.ejrad.2010.12.075. Epub 2011 Feb 4. Eur J Radiol. 2011. PMID: 21295932
-
Layered enhancement at magnetic resonance enterography in inflammatory bowel disease: A meta-analysis.World J Gastroenterol. 2019 Aug 21;25(31):4555-4566. doi: 10.3748/wjg.v25.i31.4555. World J Gastroenterol. 2019. PMID: 31496631 Free PMC article.
-
[MRI in chronic inflammatory bowel disease].Rofo. 2001 Jan;173(1):4-11. doi: 10.1055/s-2001-10224. Rofo. 2001. PMID: 11225416 Review. German.
Cited by
-
Association between body fat composition and disease duration, clinical activity, and intravenous corticosteroid-induced response in inflammatory bowel disease.Lipids Health Dis. 2023 Jul 22;22(1):106. doi: 10.1186/s12944-023-01874-4. Lipids Health Dis. 2023. PMID: 37481662 Free PMC article.
-
Magnetic resonance imaging may predict deep remission in patients with perianal fistulizing Crohn's disease.World J Gastroenterol. 2017 Jun 21;23(23):4285-4292. doi: 10.3748/wjg.v23.i23.4285. World J Gastroenterol. 2017. PMID: 28694669 Free PMC article.
-
Magnetic resonance enterography and bowel ultrasonography in Saudi Arabian patients with Crohn's disease: A correlation study.Saudi J Gastroenterol. 2022 May-Jun;28(3):186-192. doi: 10.4103/sjg.sjg_261_21. Saudi J Gastroenterol. 2022. PMID: 34380869 Free PMC article.
-
Optimized timing of using infliximab in perianal fistulizing Crohn's disease.World J Gastroenterol. 2020 Apr 14;26(14):1554-1563. doi: 10.3748/wjg.v26.i14.1554. World J Gastroenterol. 2020. PMID: 32327905 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
