

A dual tracer (68)Ga-DOTANOC PET/CT and (18)F-FDG PET/CT pilot study for detection of cardiac sarcoidosis
- PMID: 27316444
- PMCID: PMC4912521
- DOI: 10.1186/s13550-016-0207-6
A dual tracer (68)Ga-DOTANOC PET/CT and (18)F-FDG PET/CT pilot study for detection of cardiac sarcoidosis
Abstract
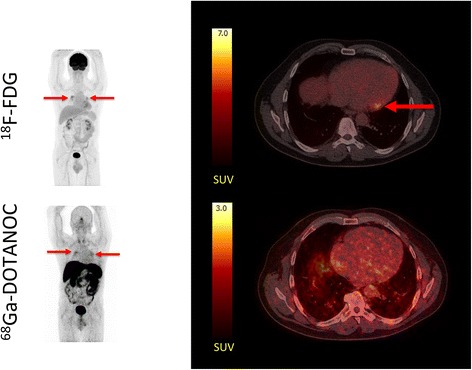
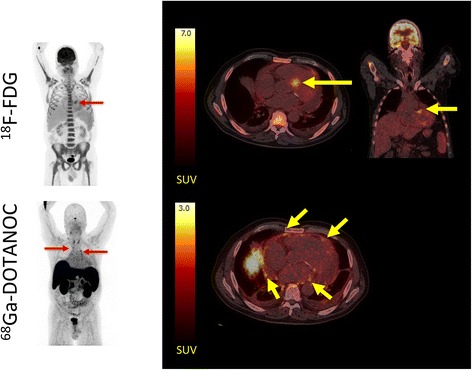
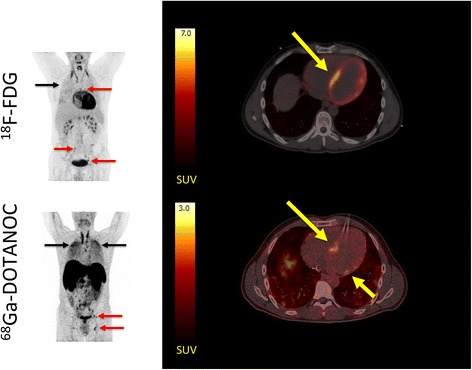
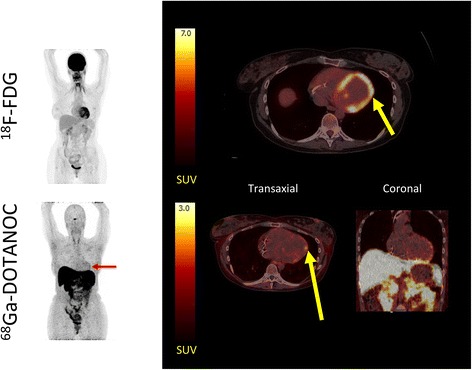
Background: Cardiac sarcoidosis (CS) is a potentially fatal condition lacking a single test with acceptable diagnostic accuracy. (18)F-FDG PET/CT has emerged as a promising imaging modality, but is challenged by physiological myocardial glucose uptake. An alternative tracer, (68)Ga-DOTANOC, binds to somatostatin receptors on inflammatory cells in sarcoid granulomas. We therefore aimed to conduct a proof-of-concept study using (68)Ga-DOTANOC to diagnose CS. In addition, we compared diagnostic accuracy and inter-observer variability of (68)Ga-DOTANOC vs. (18)F-FDG PET/CT.
Methods: Nineteen patients (seven female) with suspected CS were prospectively recruited and dual tracer scanned within 7 days. PET images were reviewed by four expert readers for signs of CS and compared to the reference standard (Japanese ministry of Health and Welfare CS criteria).
Results: CS was diagnosed in 3/19 patients. By consensus, 11/19 (18)F-FDG scans and 0/19 (68)Ga-DOTANOC scans were rated as inconclusive. The sensitivity of (18)F-FDG PET for diagnosing CS was 33 %, specificity was 88 %, PPV was 33 %, NPV was 88 %, and diagnostic accuracy was 79 %. For (68)Ga-DOTANOC, accuracy was 100 %. Inter-observer agreement was poor for (18)F-FDG PET (Fleiss' combined kappa 0.27, NS) and significantly better for (68)Ga-DOTANOC (Fleiss' combined kappa 0.46, p = 0.001).
Conclusions: Despite prolonged pre-scan fasting, a large proportion of (18)F-FDG PET/CT images were rated as inconclusive, resulting in low agreement among reviewers and correspondingly poor diagnostic accuracy. By contrast, (68)Ga-DOTANOC PET/CT had excellent diagnostic accuracy with the caveat that inter-observer variability was still significant. Nevertheless, (68)Ga-DOTANOC PET/CT looks very promising as an alternative CS PET tracer.
Trial registration: Current Controlled Trials NCT01729169 .
Keywords: Cardiac sarcoidosis; Heart failure; Inflammation; PET/CT; Somatostatin receptor imaging.
Figures

References
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
