

Web-Based Fully Automated Self-Help With Different Levels of Therapist Support for Individuals With Eating Disorder Symptoms: A Randomized Controlled Trial
- PMID: 27317358
- PMCID: PMC4930527
- DOI: 10.2196/jmir.5709
Web-Based Fully Automated Self-Help With Different Levels of Therapist Support for Individuals With Eating Disorder Symptoms: A Randomized Controlled Trial
Abstract
Background: Despite the disabling nature of eating disorders (EDs), many individuals with ED symptoms do not receive appropriate mental health care. Internet-based interventions have potential to reduce the unmet needs by providing easily accessible health care services.
Objective: This study aimed to investigate the effectiveness of an Internet-based intervention for individuals with ED symptoms, called "Featback." In addition, the added value of different intensities of therapist support was investigated.
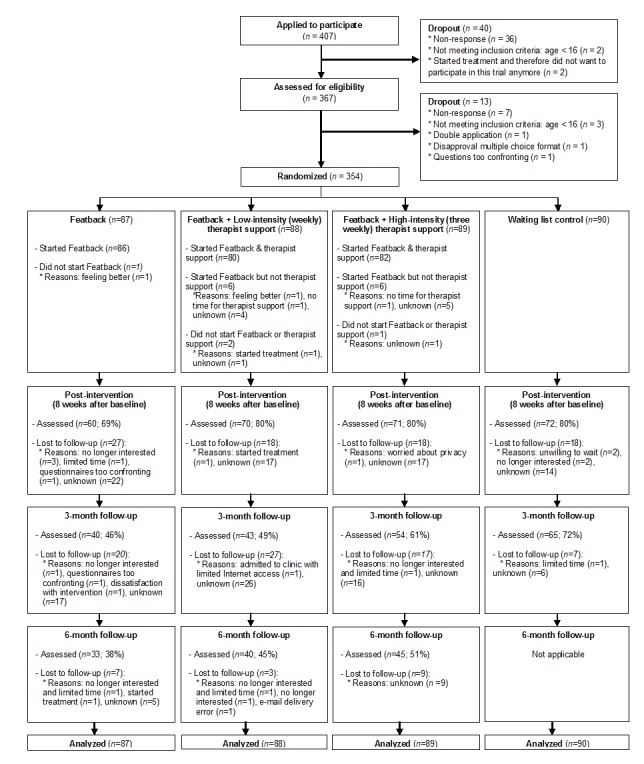
Methods: Participants (N=354) were aged 16 years or older with self-reported ED symptoms, including symptoms of anorexia nervosa, bulimia nervosa, and binge eating disorder. Participants were recruited via the website of Featback and the website of a Dutch pro-recovery-focused e-community for young women with ED problems. Participants were randomized to: (1) Featback, consisting of psychoeducation and a fully automated self-monitoring and feedback system, (2) Featback supplemented with low-intensity (weekly) digital therapist support, (3) Featback supplemented with high-intensity (3 times a week) digital therapist support, and (4) a waiting list control condition. Internet-administered self-report questionnaires were completed at baseline, post-intervention (ie, 8 weeks after baseline), and at 3- and 6-month follow-up. The primary outcome measure was ED psychopathology. Secondary outcome measures were symptoms of depression and anxiety, perseverative thinking, and ED-related quality of life. Statistical analyses were conducted according to an intent-to-treat approach using linear mixed models.
Results: The 3 Featback conditions were superior to a waiting list in reducing bulimic psychopathology (d=-0.16, 95% confidence interval (CI)=-0.31 to -0.01), symptoms of depression and anxiety (d=-0.28, 95% CI=-0.45 to -0.11), and perseverative thinking (d=-0.28, 95% CI=-0.45 to -0.11). No added value of therapist support was found in terms of symptom reduction although participants who received therapist support were significantly more satisfied with the intervention than those who did not receive supplemental therapist support. No significant differences between the Featback conditions supplemented with low- and high-intensity therapist support were found regarding the effectiveness and satisfaction with the intervention.
Conclusions: The fully automated Internet-based self-monitoring and feedback intervention Featback was effective in reducing ED and comorbid psychopathology. Supplemental therapist support enhanced satisfaction with the intervention but did not increase its effectiveness. Automated interventions such as Featback can provide widely disseminable and easily accessible care. Such interventions could be incorporated within a stepped-care approach in the treatment of EDs and help to bridge the gap between mental disorders and mental health care services.
Trial registration: Netherlands Trial Registry: NTR3646; http://www.trialregister.nl/trialreg/admin/ rctview.asp?TC=3646 (Archived by WebCite at http://www.webcitation.org/6fgHTGKHE).
Keywords: Internet-based; eating disorders; ehealth; self-help; self-monitoring; therapist support.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Hudson JI, Hiripi E, Pope HG, Kessler RC. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biol Psychiatry. 2007 Feb 1;61(3):348–58. doi: 10.1016/j.biopsych.2006.03.040. http://europepmc.org/abstract/MED/16815322 S0006-3223(06)00474-4 - DOI - PMC - PubMed
-
- Kessler RC, Berglund PA, Chiu WT, Deitz AC, Hudson JI, Shahly V, Aguilar-Gaxiola S, Alonso J, Angermeyer MC, Benjet C, Bruffaerts R, de Girolamo G, de Graaf R, Maria Haro J, Kovess-Masfety V, O'Neill S, Posada-Villa J, Sasu C, Scott K, Viana MC, Xavier M. The prevalence and correlates of binge eating disorder in the World Health Organization World Mental Health Surveys. Biol Psychiatry. 2013 May 1;73(9):904–14. doi: 10.1016/j.biopsych.2012.11.020. http://europepmc.org/abstract/MED/23290497 S0006-3223(12)01028-1 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
