

Team-based model for non-operating room airway management: validation using a simulation-based study
- PMID: 27317709
- PMCID: PMC4913398
- DOI: 10.1093/bja/aew121
Team-based model for non-operating room airway management: validation using a simulation-based study
Abstract
Background: Non-operating room (non-OR) airway management has previously been identified as an area of concern because it carries a significant risk for complications. One reason for this could be attributed to the independent practice of residents in these situations. The aim of the present study was to ascertain whether differences in performance exist between residents working alone vs with a resident partner when encountering simulated non-OR airway management scenarios.
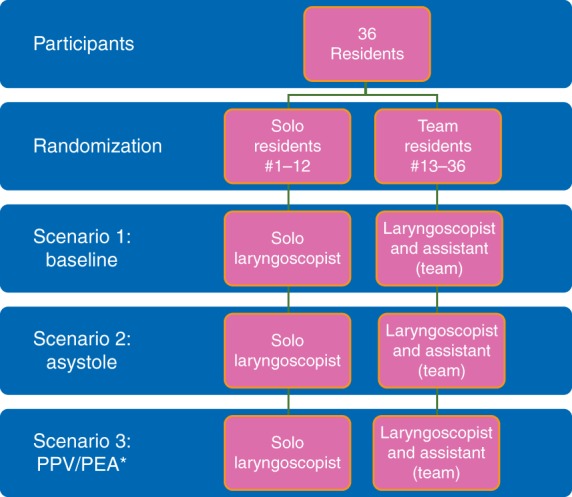
Methods: Thirty-six anaesthesia residents were randomized into two groups. Each group experienced three separate scenarios (two scenarios initially and then a third 6 weeks later). The scenarios consisted of one control scenario and two critical event scenarios [i.e. asystole during laryngoscopy and pulseless electrical activity (PEA) upon post-intubation institution of positive pressure ventilation]. One group experienced the simulated non-OR scenarios alone (Solo group). The other group consisted of resident pairs, participating in the same three scenarios (Team group).
Results: Although the time to intubation did not differ between the Solo and Team groups, there were several differences in performance. The Team group received better overall performance ratings for the asystole (8.5 vs 5.5 out of 10; P<0.001) and PEA (8.5 vs 5.8 out of 10; P<0.001) scenarios. The Team group was also able to recognize asystole and PEA conditions faster than the Solo group [10.1 vs 23.5 s (P<0.001) and 13.3 vs 36.0 s (P<0.001), respectively].
Conclusions: Residents who performed a simulated intubation with a second trained provider had better overall performance than those who practised independently. The residents who practised in a group were also faster to diagnose serious complications, including peri-intubation asystole and PEA. Given these data, it is reasonable that training programmes consider performing all non-OR airway management with a team-based method.
Keywords: airway management; high-fidelity simulation; team-based anaesthesia.
© The Author 2016. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
Comment on
-
Death and other complications of emergency airway management in critically ill adults. A prospective investigation of 297 tracheal intubations.Anesthesiology. 1995 Feb;82(2):367-76. doi: 10.1097/00000542-199502000-00007. Anesthesiology. 1995. PMID: 7856895
References
-
- Jaber S, Amraoui J, Lefrant JY et al. Clinical practice and risk factors for immediate complications of endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Crit Care Med 2006; 34: 2355–61 - PubMed
-
- Benedetto WJ, Hess DR, Gettings E et al. Urgent tracheal intubation in general hospital units: an observational study. J Clin Anesth 2007; 19: 20–4 - PubMed
-
- Martin LD, Mhyre JM, Shanks AM, Tremper KK, Kheterpal S. 3,423 emergency tracheal intubations at a university hospital: airway outcomes and complications. Anesthesiology 2011; 114: 42–8 - PubMed
-
- Peterson GN, Domino KB, Caplan RA, Posner KL, Lee LA, Cheney FW. Management of the difficult airway: a closed claims analysis. Anesthesiology 2005; 103: 33–9 - PubMed
-
- Schmidt UH, Kumwilaisak K, Bittner E, George E, Hess D. Effects of supervision by attending anesthesiologists on complications of emergency tracheal intubation. Anesthesiology 2008; 109: 973–7 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
