

Diagnostic performance of contrast-enhanced multidetector computed tomography and gadoxetic acid disodium-enhanced magnetic resonance imaging in detecting hepatocellular carcinoma: direct comparison and a meta-analysis
- PMID: 27318936
- PMCID: PMC5018023
- DOI: 10.1007/s00261-016-0807-7
Diagnostic performance of contrast-enhanced multidetector computed tomography and gadoxetic acid disodium-enhanced magnetic resonance imaging in detecting hepatocellular carcinoma: direct comparison and a meta-analysis
Abstract
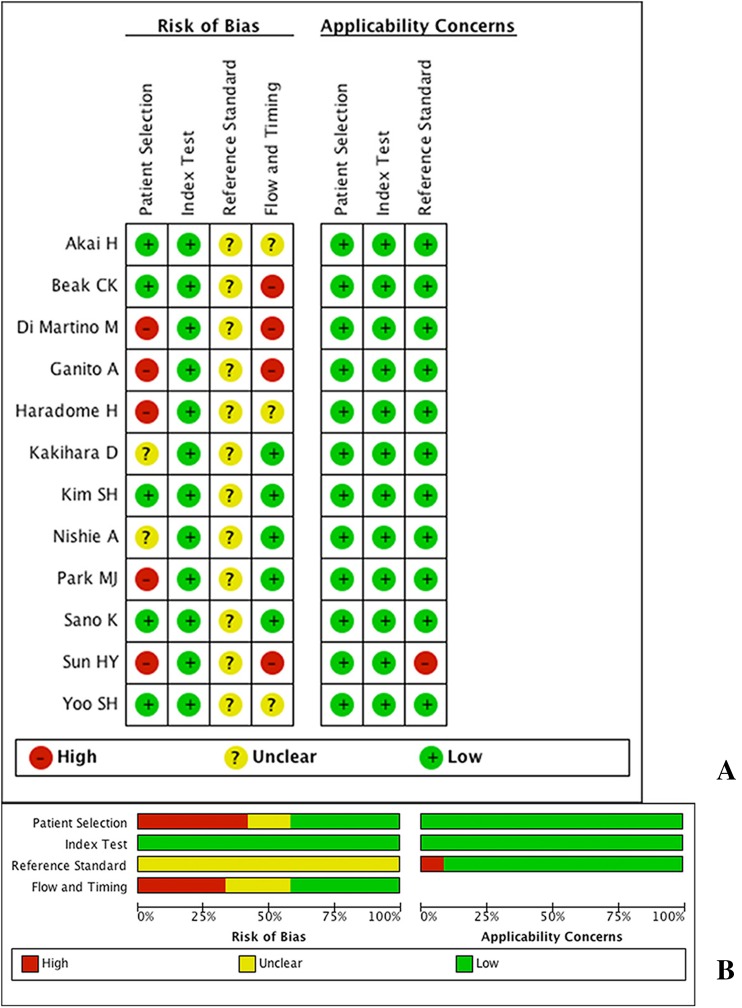
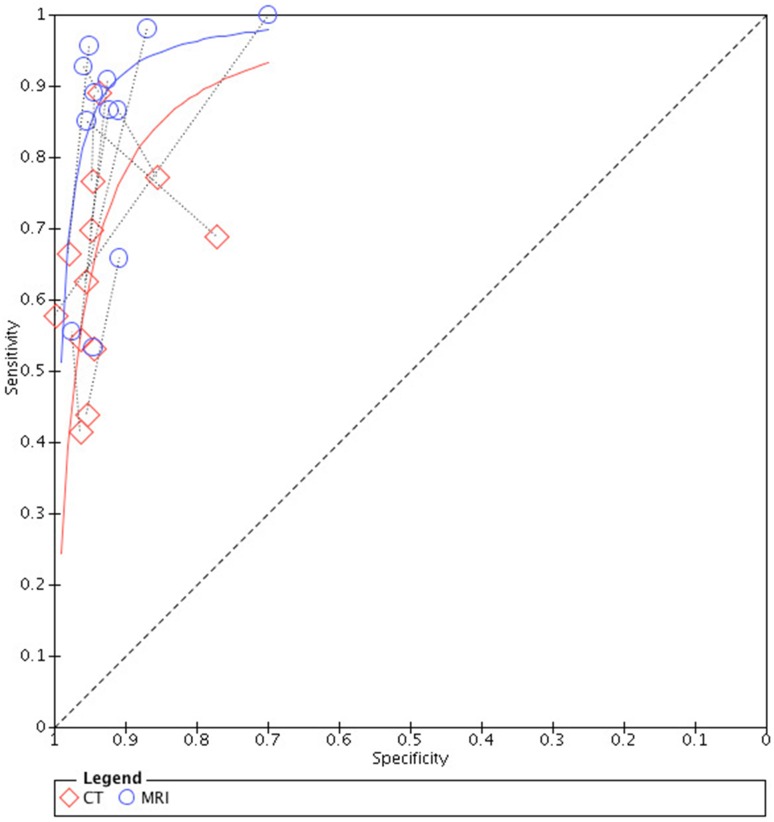
The purpose of this study was to directly (head-to-head) compare the per-lesion diagnostic performance of contrast-enhanced computed tomography (CT) (also referred to as CT hereafter) and gadoxetic acid disodium (Gd-EOB-DTPA)-enhanced magnetic resonance (MR) imaging (also referred to as MRI hereafter) for the detection of hepatocellular carcinoma (HCC). Studies reporting direct per-lesion comparison data of contrast-enhanced multidetector CT and Gd-EOB-DTPA-enhanced MR imaging that were published between January 2000 and January 2015 were analyzed. The data of each study were extracted. Systematic review, paired meta-analysis, and subgroup analysis were performed. Twelve studies including 627 patients and 793 HCC lesions were analyzed. The sensitivity estimates of MRI and CT were, respectively, 0.86 (95% CI 0.76-0.93) and 0.70 (95% CI 0.58-0.80), with significant difference (P < 0.05). The sensitivity estimates were both 0.94 (95% CI 0.92-0.96) (Chi-square 4.84, degrees of freedom = 1, P > 0.05). In all subgroups, Gd-EOB-DTPA-enhanced MR imaging was more sensitive than multidetector CT for the detection of HCC, and specificity estimates of both tests maintained at a similarly high level in all conditions: sensitivity estimates of both tests were reduced in studies where patients were diagnosed with HCC solely by liver explant or in those where HCC lesions were small (≤2 cm, especially when ≤1 cm). But in all situations, sensitivities of MRI were higher than those of CT with or without significance. Gd-EOB-DTPA-enhanced MR imaging showed better per-lesion diagnostic performance than multidetector CT for the diagnosis of HCC in patients with cirrhosis and in small hepatic lesions.
Keywords: Computed tomography; Diagnosis; Gadoxetic acid disodium-enhanced magnetic resonance imaging; Hepatocellular carcinoma; Meta-analysis.
Conflict of interest statement
Compliance with ethical standards Disclosure The scientific guarantor of this publication is JIANG Yuan Yuan. The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. The authors state that this work has not received any funding. No complex statistical methods were necessary for this paper. Conflict of Interest There are no potential conflicts of interest, and there are no fund sources for the financial support. Ethical approval This article does not contain any studies with human participants or animals performed by any of the authors. This is a diagnostic study.
Figures


References
-
- The World Health Organization. GLOBOCAN 2012. Available: http://globocan.iarc.fr/Pages/fact_sheets_canceraspx
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
