

Acute Kidney Injury Severity and Long-Term Readmission and Mortality After Cardiac Surgery
- PMID: 27319985
- PMCID: PMC5077656
- DOI: 10.1016/j.athoracsur.2016.04.020
Acute Kidney Injury Severity and Long-Term Readmission and Mortality After Cardiac Surgery
Abstract
Background: Acute kidney injury (AKI) is a common complication after cardiac surgery. While AKI severity is known to be associated with increased risk of short-term outcomes, its long-term impact is less well understood.
Methods: Adult patients undergoing isolated coronary artery bypass graft surgery at eight centers were enrolled into the Northern New England biomarker registry (n = 1,610). Patients were excluded if they had renal failure (n = 15) or died during index admission (n = 38). Severity of AKI was defined using the Acute Kidney Injury Network (AKIN). We linked our cohort to national Medicare and state all-payer claims to ascertain readmissions and to the National Death Index to ascertain survival. Kaplan-Meier and multivariate Cox proportional hazards modeling was conducted for time to readmission and death over 5 years.
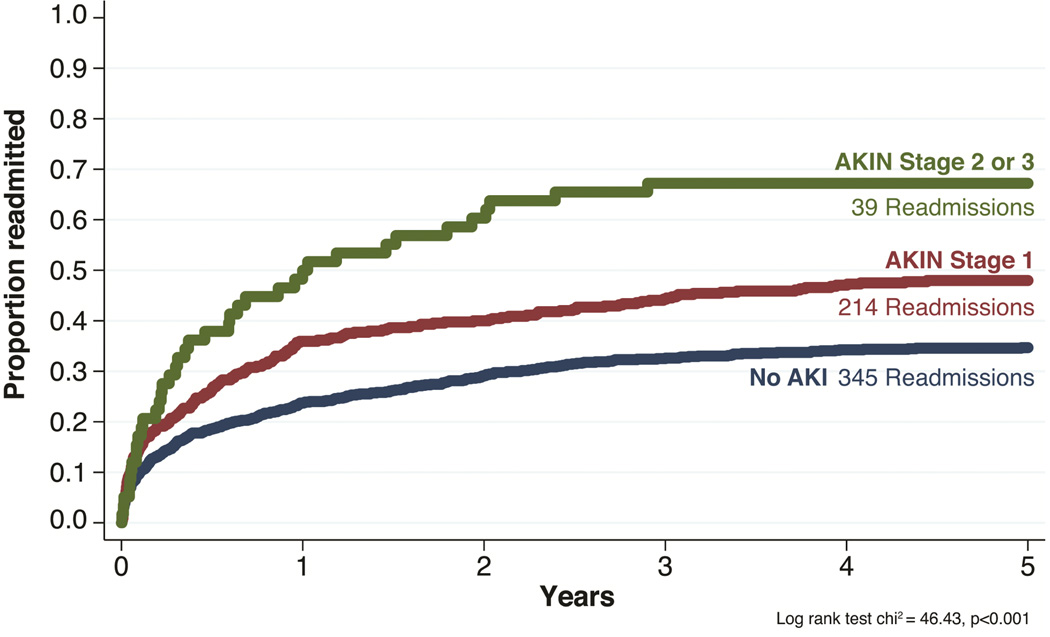
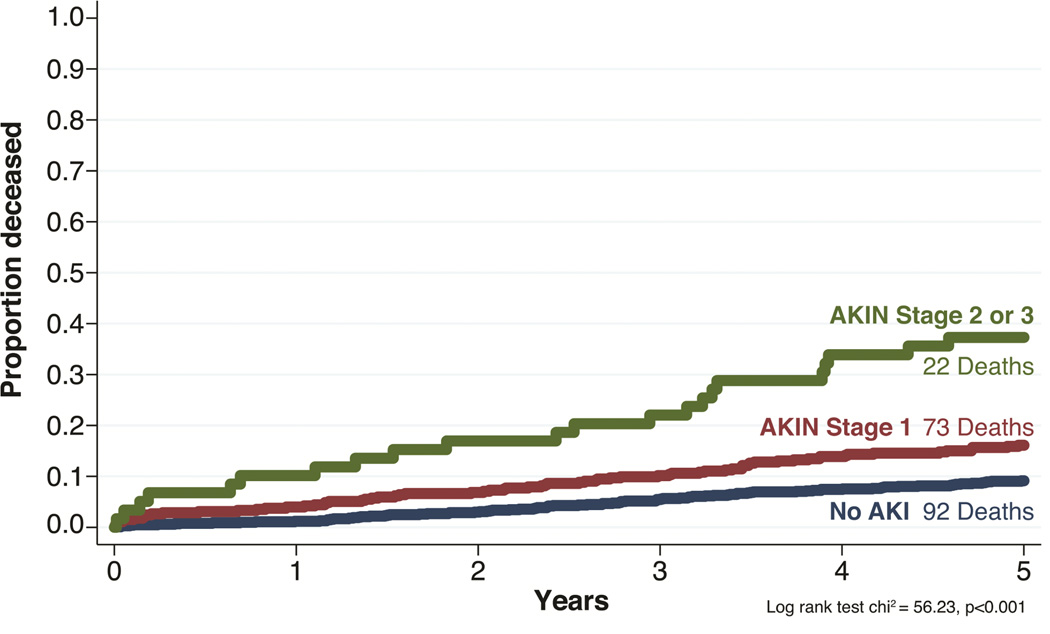
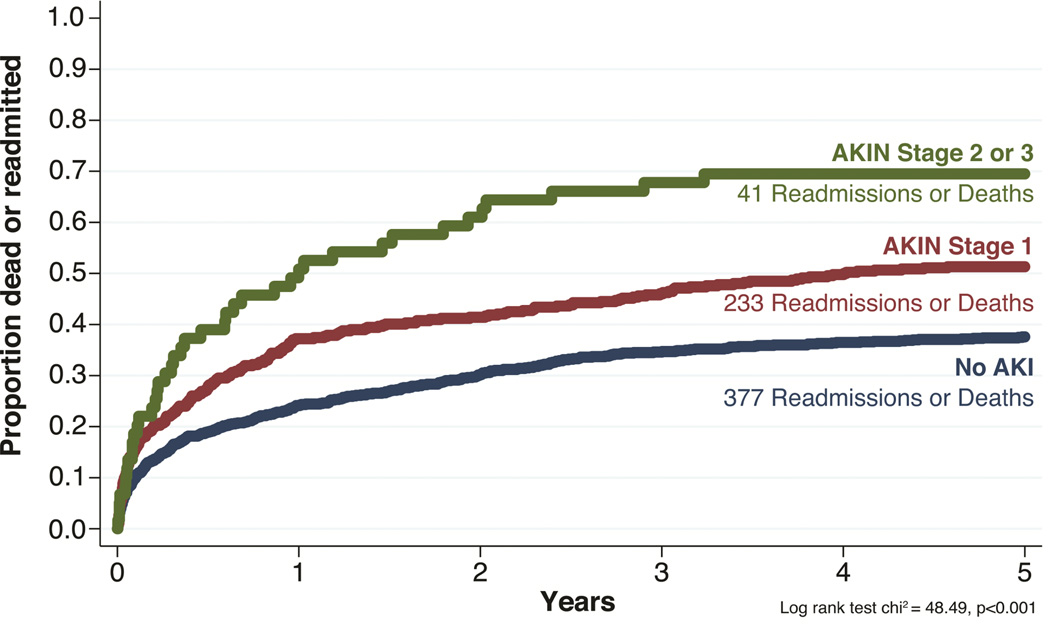
Results: Within 5 years, 513 patients (33.8%) had AKI with AKIN stage 1 (29.9%) and stage 2 to 3 (3.9%). There were 620 readmissions (39.9%) and 370 deaths (23.8%). After adjustment, stage 1 AKI patients had a 31% increased risk of readmission (95% confidence interval [CI]: 1.10 to 1.57), whereas stage 2 or 3 patients had a 98% increased risk (95% CI: 1.41 to 2.78) compared with patients having no AKI. Relative to patients without AKI, stage 1 patients had a 56% increased risk of mortality (95% CI: 1.14 to 2.13), whereas stage 2 or 3 patients had a 3.5 times higher risk (95% CI: 2.16 to 5.60).
Conclusions: Severity of AKI using the AKIN stage criteria is associated with a significantly increased risk of 5-year readmission and mortality. Our findings suggest that efforts to reduce AKI in the perioperative period may have a significant long-term impact on patients and payers in reducing mortality and health care utilization.
Copyright © 2016 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Brock J, Mitchell J, Irby K, et al. Association between quality improvement for care transitions in communities and rehospitalizations among medicare beneficiaries. JAMA : the journal of the American Medical Association. 2013;309(4):381–391. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the medicare fee-forservice program. N Engl J Med. 2009;360(14):1418–1428. - PubMed
-
- Litmathe J, Kurt M, Feindt P, Gams E, Boeken U. Predictors and outcome of icu readmission after cardiac surgery. Thorac Cardiovasc Surg. 2009;57(7):391–394. - PubMed
-
- Angelelli J, Gifford D, Intrator O, Gozalo P, Laliberte L, Mor V. Access to postacute nursing home care before and after the bba. Balanced budget act. Health Aff (Millwood) 2002;21(5):254–264. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
