

The use of green tea polyphenols for treating residual albuminuria in diabetic nephropathy: A double-blind randomised clinical trial
- PMID: 27320846
- PMCID: PMC4913255
- DOI: 10.1038/srep28282
The use of green tea polyphenols for treating residual albuminuria in diabetic nephropathy: A double-blind randomised clinical trial
Abstract
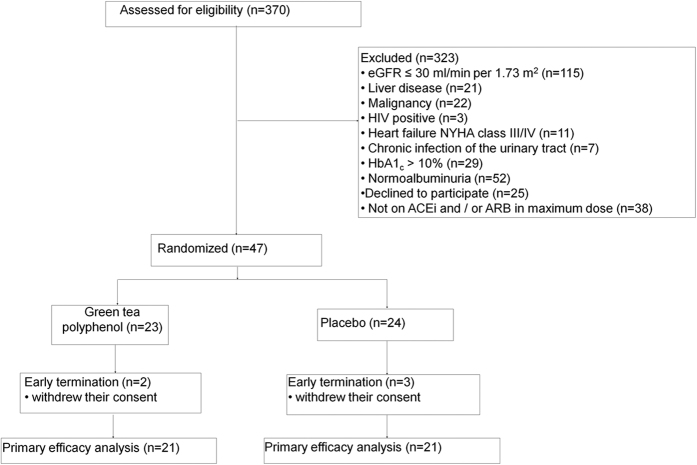
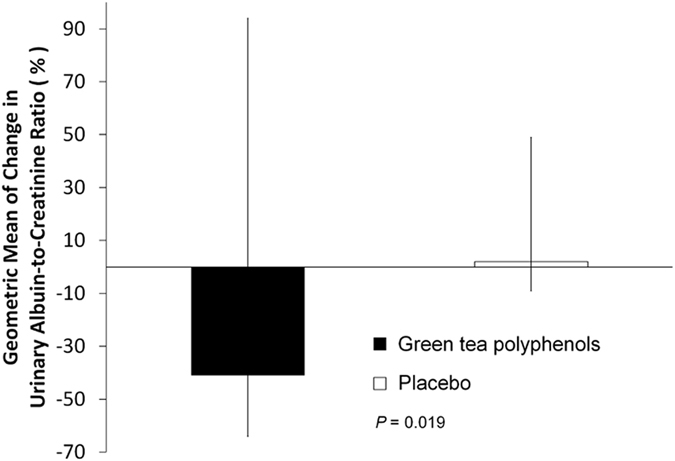
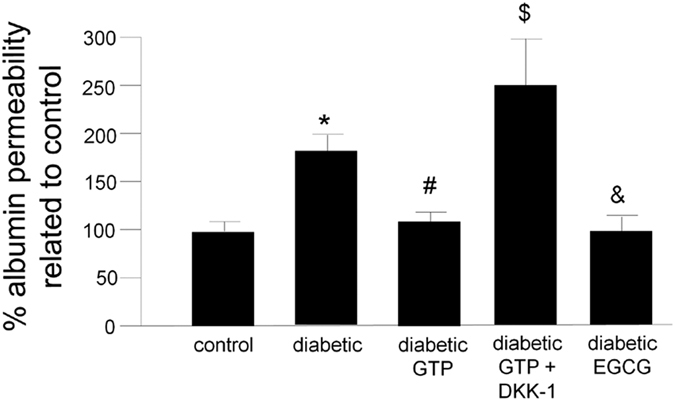
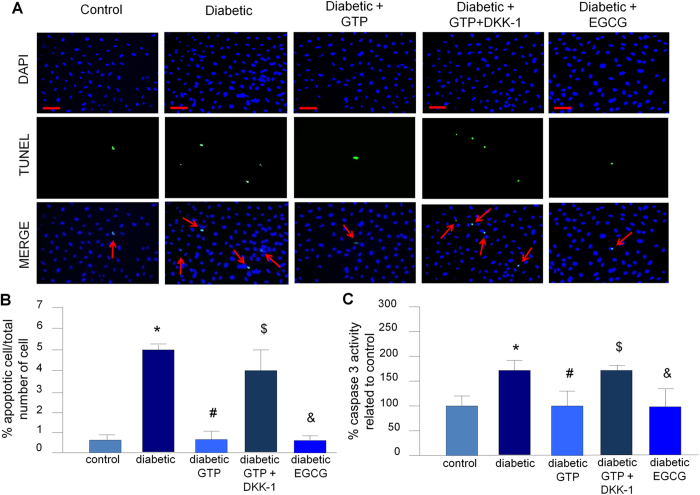
Prior research has shown that in experimental diabetes mellitus, green tea reduces albuminuria by decreasing podocyte apoptosis through activation of the WNT pathway. We investigated the effect of green tea polyphenols (GTP) on residual albuminuria of diabetic subjects with nephropathy. We conducted a randomised, double-blind study in 42 diabetic subjects with a urinary albumin-creatinine ratio (UACR) >30 mg/g, despite administration of the maximum recommended dose of renin-angiotensin (RAS) inhibition. Patients were randomly assigned to two equal groups to receive either GTP (containing 800 mg of epigallocatechin gallate, 17 with type 2 diabetes and 4 with type 1 diabetes) or placebo (21 with type 2 diabetes) for 12 weeks. Treatment with GTP reduced UACR by 41%, while the placebo group saw a 2% increase in UACR (p = 0.019). Podocyte apoptosis (p = 0.001) and in vitro albumin permeability (p < 0.001) were higher in immortalized human podocytes exposed to plasma from diabetic subjects compared to podocytes treated with plasma from normal individuals. In conclusion, GTP administration reduces albuminuria in diabetic patients receiving the maximum recommended dose of RAS. Reduction in podocyte apoptosis by activation of the WNT pathway may have contributed to this effect.
Figures
References
-
- Gaede P., Vedel P., Parving H. H. & Pedersen O. Intensified multifactorial intervention in patients with type 2 diabetes mellitus and microalbuminuria: the Steno type 2 randomised study. Lancet 353, 617–622 (1999). - PubMed
-
- De Zeeuw D. et al.. Albuminuria, a therapeutic target for cardiovascular protection in type 2 diabetic patients with nephropathy. Circulation 110, 921–927 (2004). - PubMed
-
- Holtkamp F. A. et al.. Albuminuria and blood pressure, independent targets for cardioprotective therapy in patients with diabetes and nephropathy. Eur. Heart J. 32, 1493–1499 (2011). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
