

New milestones ahead in complement-targeted therapy
- PMID: 27321574
- PMCID: PMC5404743
- DOI: 10.1016/j.smim.2016.06.001
New milestones ahead in complement-targeted therapy
Abstract
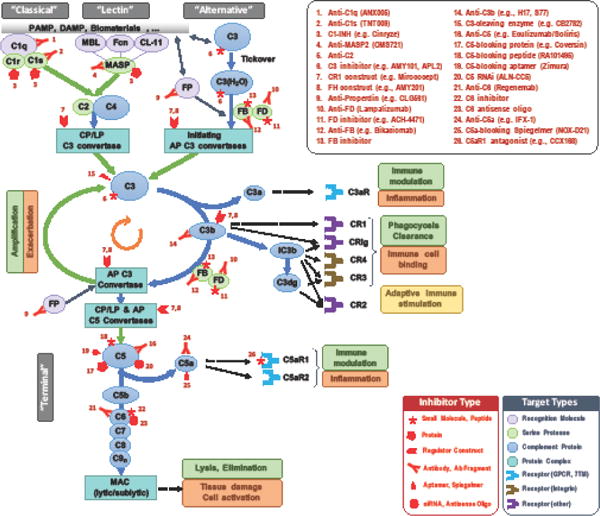
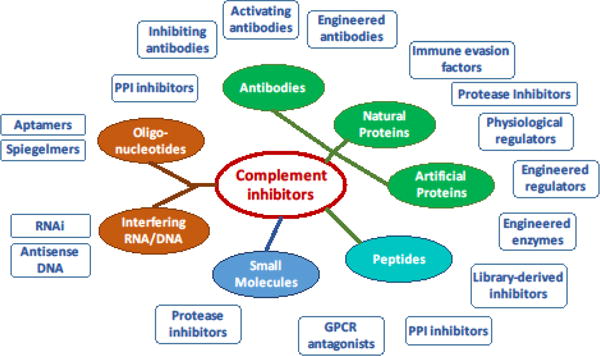
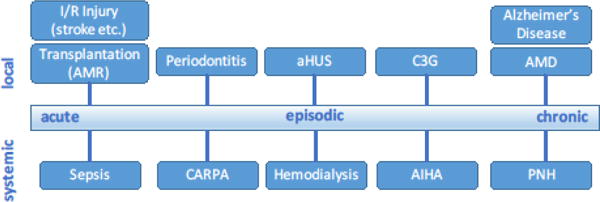
The complement system is a powerful effector arm of innate immunity that typically confers protection from microbial intruders and accumulating debris. In many clinical situations, however, the defensive functions of complement can turn against host cells and induce or exacerbate immune, inflammatory, and degenerative conditions. Although the value of inhibiting complement in a therapeutic context has long been recognized, bringing complement-targeted drugs into clinical use has proved challenging. This important milestone was finally reached a decade ago, yet the clinical availability of complement inhibitors has remained limited. Still, the positive long-term experience with complement drugs and their proven effectiveness in various diseases has reinvigorated interest and confidence in this approach. Indeed, a broad variety of clinical candidates that act at almost any level of the complement activation cascade are currently in clinical development, with several of them being evaluated in phase 2 and phase 3 trials. With antibody-related drugs dominating the panel of clinical candidates, the emergence of novel small-molecule, peptide, protein, and oligonucleotide-based inhibitors offers new options for drug targeting and administration. Whereas all the currently approved and many of the proposed indications for complement-targeted inhibitors belong to the rare disease spectrum, these drugs are increasingly being evaluated for more prevalent conditions. Fortunately, the growing experience from preclinical and clinical use of therapeutic complement inhibitors has enabled a more evidence-based assessment of suitable targets and rewarding indications as well as related technical and safety considerations. This review highlights recent concepts and developments in complement-targeted drug discovery, provides an overview of current and emerging treatment options, and discusses the new milestones ahead on the way to the next generation of clinically available complement therapeutics.
Keywords: Complement; Immune modulation; Inflammation; Therapeutics.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Therapeutic control of complement activation at the level of the central component C3.Immunobiology. 2016 Jun;221(6):740-6. doi: 10.1016/j.imbio.2015.06.012. Epub 2015 Jun 10. Immunobiology. 2016. PMID: 26101137 Free PMC article. Review.
-
The renaissance of complement therapeutics.Nat Rev Nephrol. 2018 Jan;14(1):26-47. doi: 10.1038/nrneph.2017.156. Epub 2017 Dec 4. Nat Rev Nephrol. 2018. PMID: 29199277 Free PMC article. Review.
-
Complement-targeted therapeutics: Are we there yet, or just getting started?Eur J Immunol. 2024 Dec;54(12):e2350816. doi: 10.1002/eji.202350816. Epub 2024 Sep 12. Eur J Immunol. 2024. PMID: 39263829 Free PMC article. Review.
-
From orphan drugs to adopted therapies: Advancing C3-targeted intervention to the clinical stage.Immunobiology. 2016 Oct;221(10):1046-57. doi: 10.1016/j.imbio.2016.06.013. Epub 2016 Jun 16. Immunobiology. 2016. PMID: 27353192 Free PMC article. Review.
-
Manipulating the mediator: modulation of the alternative complement pathway C3 convertase in health, disease and therapy.Immunobiology. 2012 Nov;217(11):1057-66. doi: 10.1016/j.imbio.2012.07.016. Immunobiology. 2012. PMID: 22964231 Free PMC article. Review.
Cited by
-
Absence of recipient C3aR1 signaling limits expansion and differentiation of alloreactive CD8+ T cell immunity and prolongs murine cardiac allograft survival.Am J Transplant. 2019 Jun;19(6):1628-1640. doi: 10.1111/ajt.15222. Epub 2019 Jan 14. Am J Transplant. 2019. PMID: 30565852 Free PMC article.
-
Therapeutic Approaches with Intravitreal Injections in Geographic Atrophy Secondary to Age-Related Macular Degeneration: Current Drugs and Potential Molecules.Int J Mol Sci. 2019 Apr 4;20(7):1693. doi: 10.3390/ijms20071693. Int J Mol Sci. 2019. PMID: 30987401 Free PMC article. Review.
-
Treatment of Rare Inflammatory Kidney Diseases: Drugs Targeting the Terminal Complement Pathway.Front Immunol. 2020 Dec 10;11:599417. doi: 10.3389/fimmu.2020.599417. eCollection 2020. Front Immunol. 2020. PMID: 33362783 Free PMC article. Review.
-
Significance of Complement System in Ischemic Stroke: A Comprehensive Review.Aging Dis. 2019 Apr 1;10(2):429-462. doi: 10.14336/AD.2019.0119. eCollection 2019 Apr. Aging Dis. 2019. PMID: 31011487 Free PMC article. Review.
-
Identification of complement inhibitory activities of two chemotherapeutic agents using a high-throughput cell imaging-based screening assay.Mol Immunol. 2018 Sep;101:86-91. doi: 10.1016/j.molimm.2018.06.009. Epub 2018 Jun 15. Mol Immunol. 2018. PMID: 29909366 Free PMC article.
References
-
- Baker BR, Erickson EH. Irreversible enzyme inhibitors. CLII. Proteolytic enzymes. X. Inhibition of guinea pig complement by substituted benzamidines. J Med Chem. 1969;12:408–414. - PubMed
-
- Muller-Eberhard HJ. Chemistry and reaction mechanisms of complement. Adv Immunol. 1968;8:1–80. - PubMed
-
- Lachmann PJ, Smith RA. Taking complement to the clinic–has the time finally come? Scand. J Immunol. 2009;69:471–478. - PubMed
-
- Sahu A, Lambris JD. Complement inhibitors: a resurgent concept in anti-inflammatory therapeutics. Immunopharmacology. 2000;49:133–148. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
