

Patients with Parkinson's Disease Show Impaired Use of Priors in Conditions of Sensory Uncertainty
- PMID: 27322000
- PMCID: PMC5633083
- DOI: 10.1016/j.cub.2016.05.039
Patients with Parkinson's Disease Show Impaired Use of Priors in Conditions of Sensory Uncertainty
Abstract
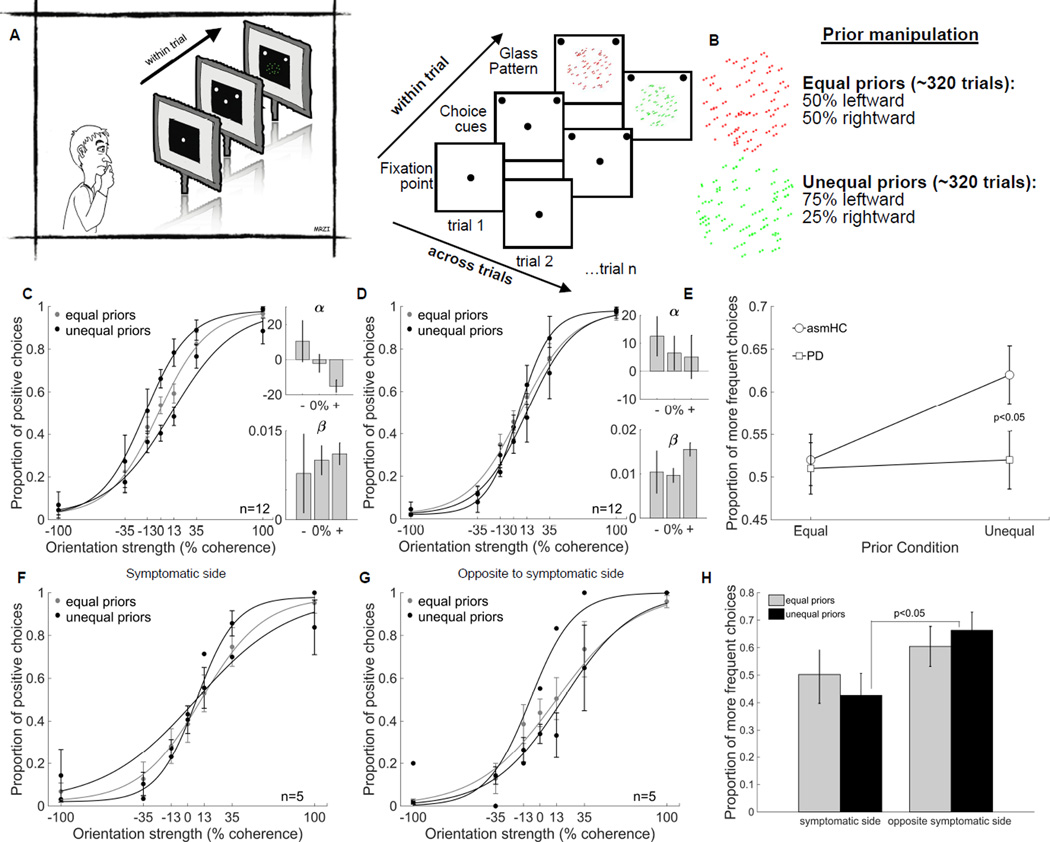
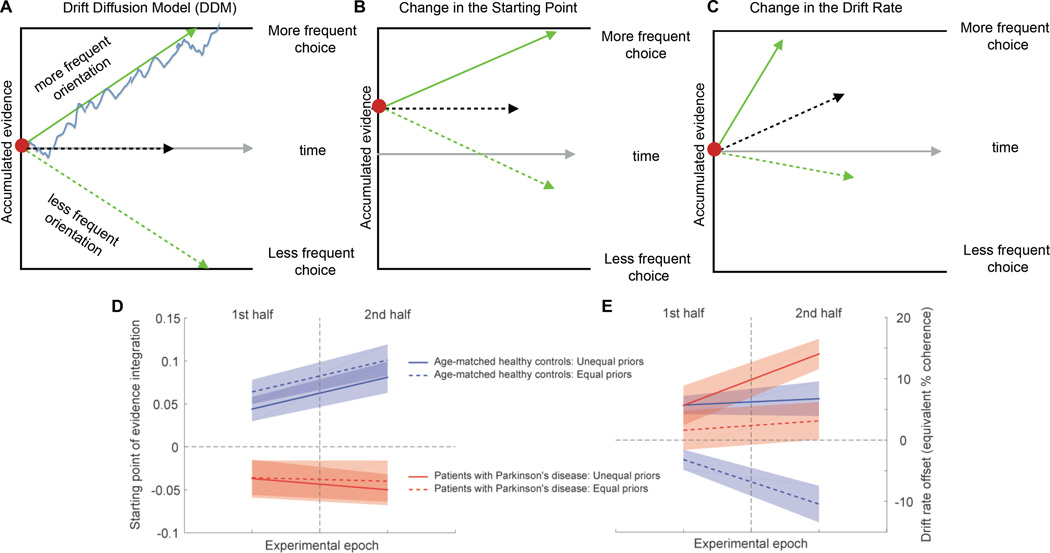
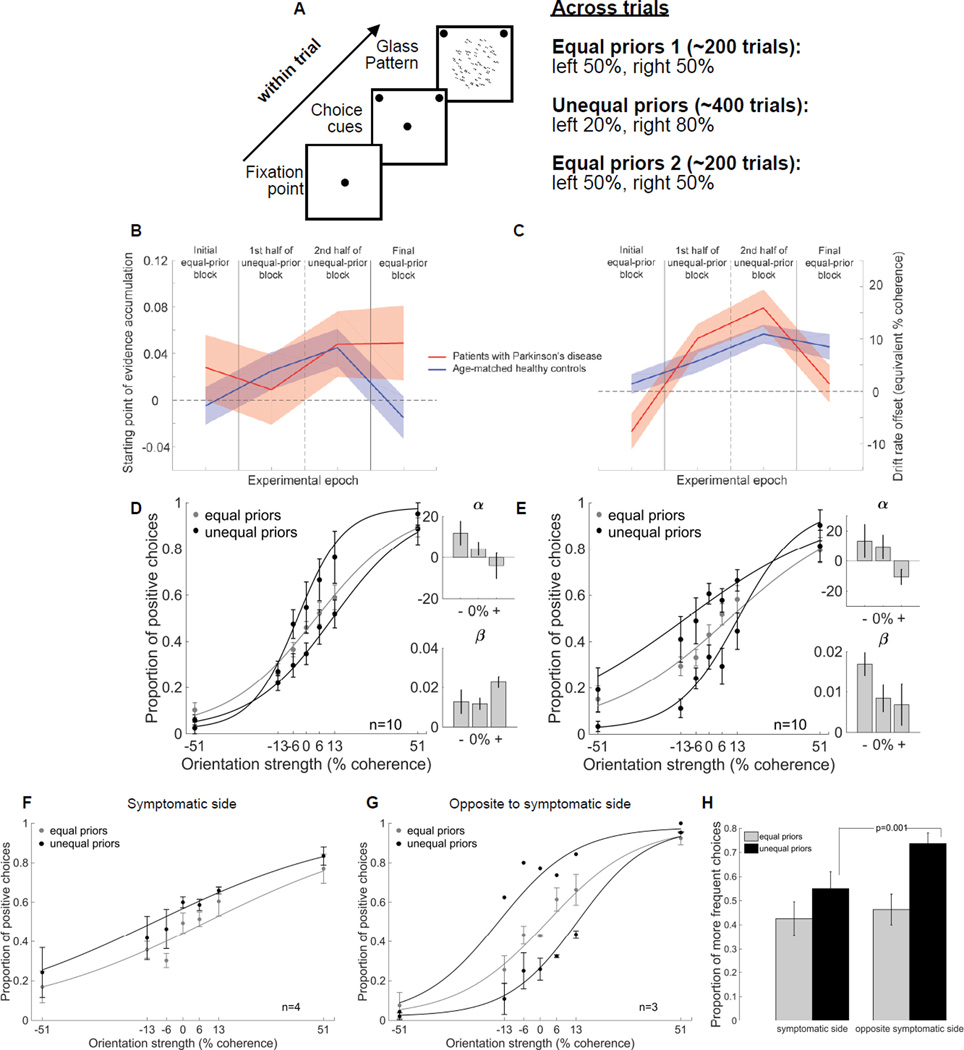
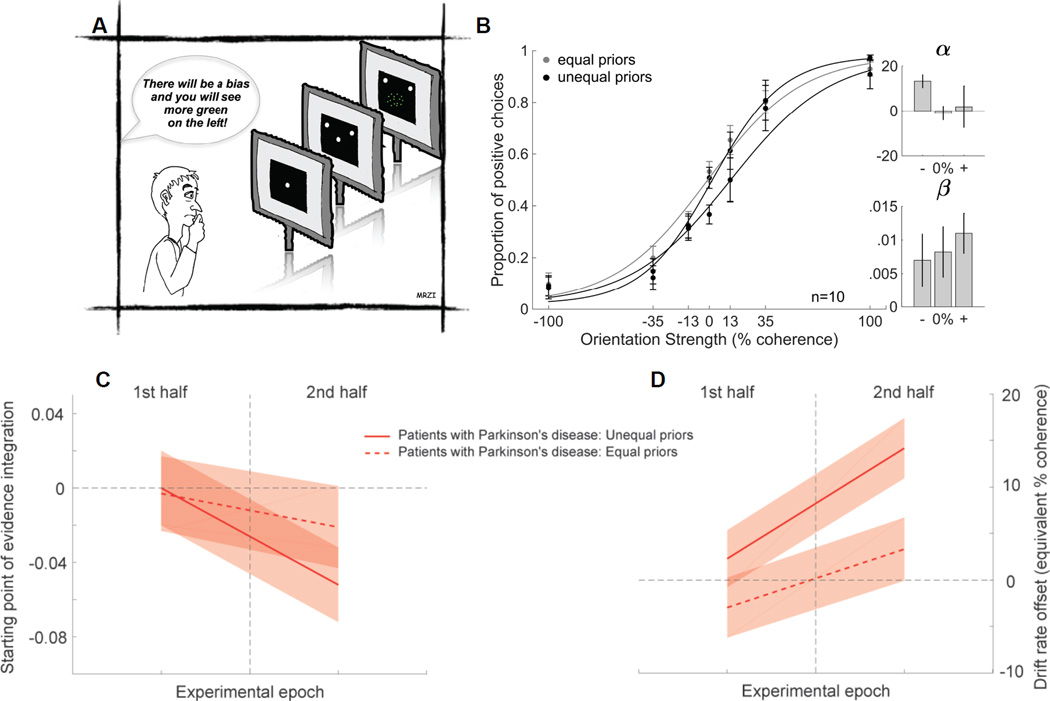
Perceptual decisions arise after considering the available sensory evidence [1]. When sensory information is unreliable, a good strategy is to rely on previous experience in similar situations to guide decisions [2-6]. It is well known that patients with Parkinson's disease (PD) are impaired at value-based decision-making [7-11]. How patients combine past experience and sensory information to make perceptual decisions is unknown. We developed a novel, perceptual decision-making task and manipulated the statistics of the sensory stimuli presented to patients with PD and healthy participants to determine the influence of past experience on decision-making. We show that patients with PD are impaired at combining previously learned information with current sensory information to guide decisions. We modeled the results using the drift-diffusion model (DDM) and found that the impairment corresponds to a failure in adjusting the amount of sensory evidence needed to make a decision. Our modeling results also show that two complementary mechanisms operate to implement a bias when two sets of priors are learned concurrently. Asymmetric decision threshold adjustments, as reflected by changes in the starting point of evidence accumulation, are responsible for a general choice bias, whereas the adjustment of a dynamic bias that develops over the course of a trial, as reflected by a drift-rate offset, provides the stimulus-specific component of the prior. A proper interplay between these two processes is required to implement a bias based on concurrent, stimulus-specific priors in decision-making. We show here that patients with PD are impaired in these across-trial decision threshold adjustments.
Keywords: Glass patterns; basal ganglia; bias; cognition; decision-making; drift-diffusion model; expectancy; implicit learning; memory; perception.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Neuroscience: Impaired Decision-Making in Parkinson's Disease.Curr Biol. 2016 Jul 25;26(14):R671-3. doi: 10.1016/j.cub.2016.05.075. Curr Biol. 2016. PMID: 27458912 Free PMC article.
References
-
- Gold JI, Shadlen MN. The neural basis of decision making. Annual Review of Neuroscience. 2007;30:535–574. - PubMed
-
- Leite F, Ratcliff R. What cognitive processes drive response biases? A diffusion model analysis. Judgement and Decision Making. 2011;6:651–687.
-
- Summerfield C, Egner T. Expectation (and attention) in visual cognition. Trends in Cognitive Sciences. 2009;13:403–409. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
