

Urinary Metabolomics Identifies a Molecular Correlate of Interstitial Cystitis/Bladder Pain Syndrome in a Multidisciplinary Approach to the Study of Chronic Pelvic Pain (MAPP) Research Network Cohort
- PMID: 27322470
- PMCID: PMC4909380
- DOI: 10.1016/j.ebiom.2016.03.040
Urinary Metabolomics Identifies a Molecular Correlate of Interstitial Cystitis/Bladder Pain Syndrome in a Multidisciplinary Approach to the Study of Chronic Pelvic Pain (MAPP) Research Network Cohort
Abstract
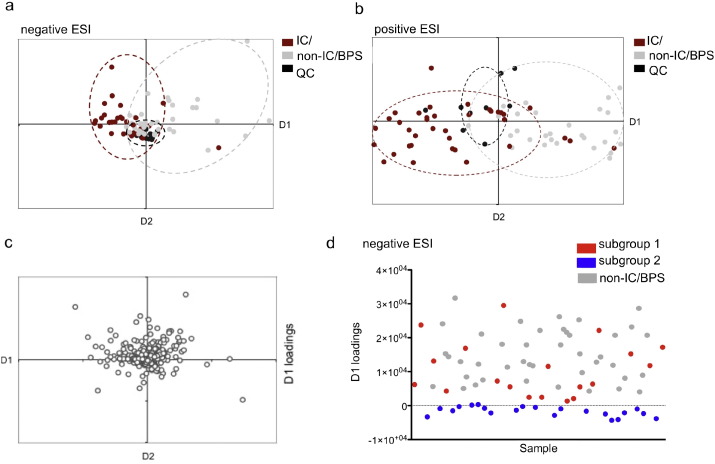
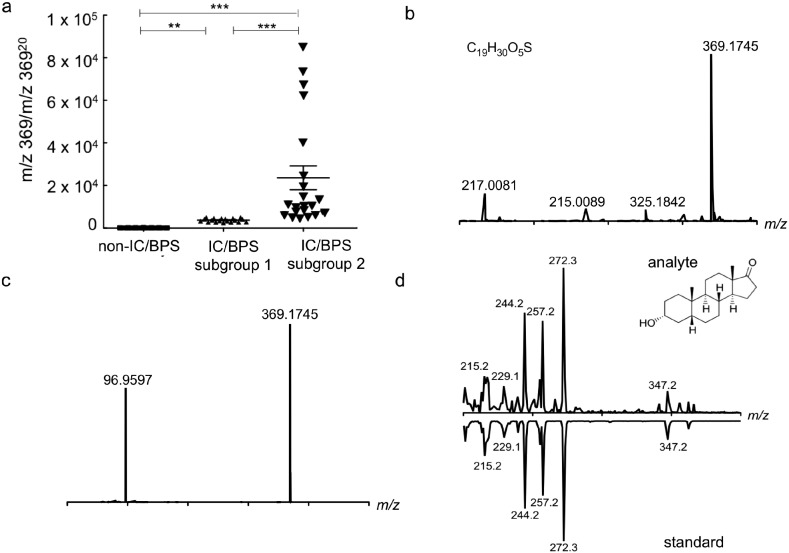
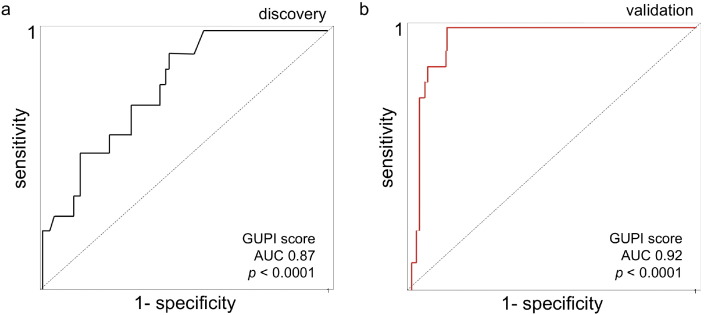
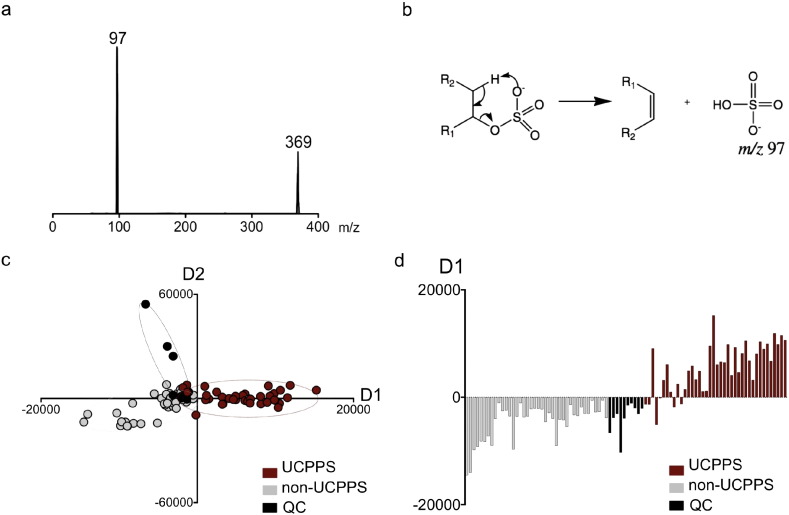
Interstitial cystitis/bladder pain syndrome (IC/BPS) is a poorly understood syndrome affecting up to 6.5% of adult women in the U.S. The lack of broadly accepted objective laboratory markers for this condition hampers efforts to diagnose and treat this condition. To identify biochemical markers for IC/BPS, we applied mass spectrometry-based global metabolite profiling to urine specimens from a cohort of female IC/BPS subjects from the Multidisciplinary Approach to the Study of Chronic Pelvic Pain (MAPP) Research Network. These analyses identified multiple metabolites capable of discriminating IC/BPS and control subjects. Of these candidate markers, etiocholan-3α-ol-17-one sulfate (Etio-S), a sulfoconjugated 5-β reduced isomer of testosterone, distinguished female IC/BPS and control subjects with a sensitivity and specificity >90%. Among IC/BPS subjects, urinary Etio-S levels are correlated with elevated symptom scores (symptoms, pelvic pain, and number of painful body sites) and could resolve high- from low-symptom IC/BPS subgroups. Etio-S-associated biochemical changes persisted through 3-6months of longitudinal follow up. These results raise the possibility that an underlying biochemical abnormality contributes to symptoms in patients with severe IC/BPS.
Copyright © 2016 The Authors. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Pain: MAPPing metabolomic markers for IC/BPS.Nat Rev Urol. 2016 Jun;13(6):300. doi: 10.1038/nrurol.2016.81. Epub 2016 Apr 26. Nat Rev Urol. 2016. PMID: 27112390 No abstract available.
Similar articles
-
Urine nerve growth factor (NGF) level, bladder nerve staining and symptom/problem scores in patients with interstitial cystitis.Adv Clin Exp Med. 2018 Feb;27(2):159-163. doi: 10.17219/acem/69231. Adv Clin Exp Med. 2018. PMID: 29521057
-
Urinary nerve growth factor level is increased in patients with interstitial cystitis/bladder pain syndrome and decreased in responders to treatment.BJU Int. 2009 Nov;104(10):1476-81. doi: 10.1111/j.1464-410X.2009.08675.x. Epub 2009 Jun 12. BJU Int. 2009. PMID: 19522864
-
Sensory mapping of pelvic dermatomes in women with interstitial cystitis/bladder pain syndrome.Neurourol Urodyn. 2018 Jan;37(1):458-465. doi: 10.1002/nau.23330. Epub 2017 Jun 19. Neurourol Urodyn. 2018. PMID: 28628232 Free PMC article.
-
Update on Urinary Tract Markers in Interstitial Cystitis/Bladder Pain Syndrome.Female Pelvic Med Reconstr Surg. 2016 Jan-Feb;22(1):16-23. doi: 10.1097/SPV.0000000000000224. Female Pelvic Med Reconstr Surg. 2016. PMID: 26571430 Review.
-
Urinary IL-33 and galectin-3 increase in patients with interstitial cystitis/bladder pain syndrome (review).Georgian Med News. 2014 Jul-Aug;(232-233):12-5. Georgian Med News. 2014. PMID: 25214264 Review.
Cited by
-
In-depth characterisation of the urine metabolome in cats with and without urinary tract diseases.Metabolomics. 2022 Mar 17;18(4):19. doi: 10.1007/s11306-022-01877-9. Metabolomics. 2022. PMID: 35305176 Free PMC article.
-
Biomarkers in the diagnosis and symptom assessment of patients with bladder pain syndrome: a systematic review.Int Urogynecol J. 2019 Nov;30(11):1785-1794. doi: 10.1007/s00192-019-04075-9. Epub 2019 Aug 13. Int Urogynecol J. 2019. PMID: 31410520
-
Peptidomics analysis reveals changes in small urinary peptides in patients with interstitial cystitis/bladder pain syndrome.Sci Rep. 2022 May 18;12(1):8289. doi: 10.1038/s41598-022-12197-2. Sci Rep. 2022. PMID: 35585122 Free PMC article.
-
The Metabolomics of Chronic Pain Conditions: A Systematic Review.Biol Res Nurs. 2020 Oct;22(4):458-471. doi: 10.1177/1099800420941105. Epub 2020 Jul 15. Biol Res Nurs. 2020. PMID: 32666804 Free PMC article.
-
Leveraging Human Microbiome Features to Diagnose and Stratify Children with Irritable Bowel Syndrome.J Mol Diagn. 2019 May;21(3):449-461. doi: 10.1016/j.jmoldx.2019.01.006. Epub 2019 Apr 17. J Mol Diagn. 2019. PMID: 31005411 Free PMC article.
References
-
- Argade S., Shaw T., Su Y., Parsons C.L. Tamm–Horsfall protein-associated nucleotides in patients with interstitial cystitis. BJU Int. 2013;111:811–819. - PubMed
-
- Bagarinao E., Johnson K.A., Martucci K.T., Ichesco E., Farmer M.A., Labus J., Ness T.J., Harris R., Deutsch G., Apkarian A.V., Mayer E.A., Clauw D.J., Mackey S. Preliminary structural MRI based brain classification of chronic pelvic pain: a MAPP network study. Pain. 2014;155:2502–2509. - PMC - PubMed
-
- Clemens J.Q. Male and female pelvic pain disorders—is it all in their heads? J. Urol. 2008;179:813–814. - PubMed
-
- Clemens J.Q., Calhoun E.A., Litwin M.S., Mcnaughton-Collins M., Kusek J.W., Crowley E.M., Landis J.R., Urologic Pelvic Pain Collaborative Research, N. Validation of a modified National Institutes of Health chronic prostatitis symptom index to assess genitourinary pain in both men and women. Urology. 2009;74:983–987. quiz 987 e1–3. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
