

Association Between Medicare Accountable Care Organization Implementation and Spending Among Clinically Vulnerable Beneficiaries
- PMID: 27322485
- PMCID: PMC4969198
- DOI: 10.1001/jamainternmed.2016.2827
Association Between Medicare Accountable Care Organization Implementation and Spending Among Clinically Vulnerable Beneficiaries
Retracted and republished in
-
Notice of Retraction and Replacement: Colla et al. Association between Medicare accountable care organization implementation and spending among clinically vulnerable beneficiaries. JAMA Internal Medicine. 2016;176(8):1167-1175.JAMA Intern Med. 2017 Nov 1;177(11):1702-1703. doi: 10.1001/jamainternmed.2017.4130. JAMA Intern Med. 2017. PMID: 28892536 No abstract available.
Abstract
Importance: Accountable care contracts hold physician groups financially responsible for the quality and cost of health care delivered to patients. Focusing on clinically vulnerable patients, those with serious conditions who are responsible for the greatest proportion of spending, may result in the largest effects on both patient outcomes and financial rewards for participating physician groups.
Objective: To estimate the effect of Medicare accountable care organization (ACO) contracts on spending and high-cost institutional use for all Medicare beneficiaries and for clinically vulnerable beneficiaries.
Design, setting, and participants: For this cohort study, 2 study populations were defined: the overall Medicare population and the clinically vulnerable subgroup of Medicare beneficiaries. The overall Medicare population was based on a random 40% sample drawn from continuously enrolled fee-for-service beneficiaries with at least 1 evaluation and management visit in a calendar year. The clinically vulnerable study population included all Medicare beneficiaries 66 years or older who had at least 3 Hierarchical Condition Categories (HCCs). Beneficiaries entered the cohort during the quarter between January 2009 to December 2011 when they first had at least 3 HCCs and remained in the cohort until death. Cohort entry was restricted to the preperiod to account for potential changes in coding practices after ACO implementation. Difference-in-difference estimations were used to compare changes in health care outcomes for Medicare beneficiaries attributed to physicians in ACOs with those attributed to non-ACO physicians from January 2009 to December 2013.
Exposures: Medicare ACOs beginning contracts in January 2012, April 2012, July 2012, and January 2013 through the Pioneer and Medicare Shared Savings Programs.
Main outcomes and measures: Total spending per beneficiary-quarter, spending categories, use of hospitals and emergency departments, ambulatory care sensitive admissions, and 30-day readmissions.
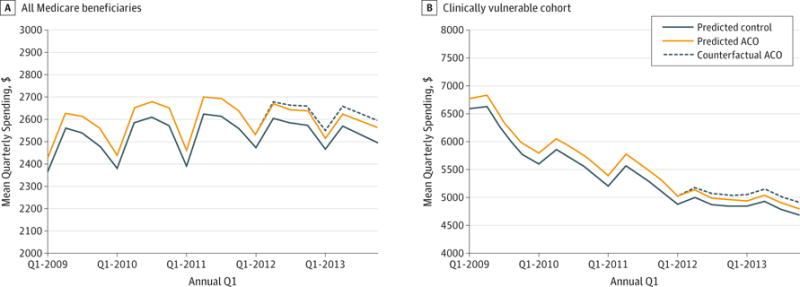
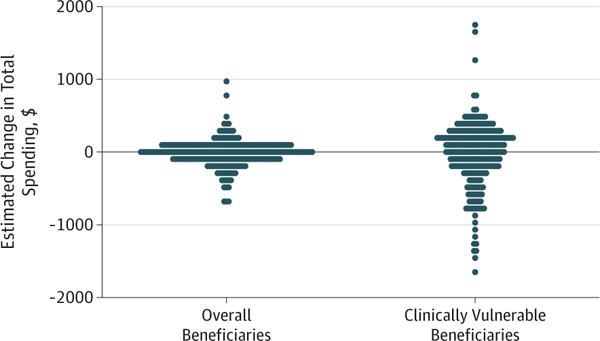
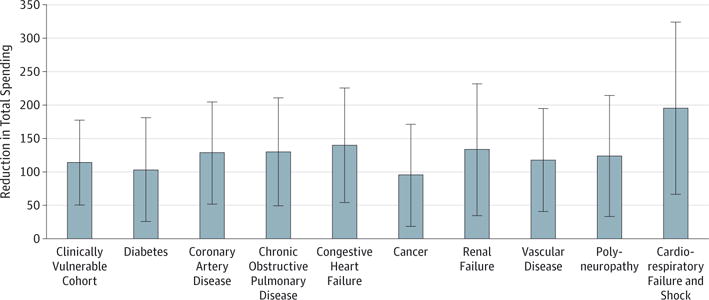
Results: Total spending decreased by $34 (95% CI, -$52 to -$15) per beneficiary-quarter after ACO contract implementation across the overall Medicare population (n = 15 592 600) and decreased $114 in clinically vulnerable patients (n = 8 673 823) (95% CI, -$178 to -$50). In the overall Medicare cohort, hospitalizations and emergency department visits decreased by 1.3 and 3.0 events per 1000 beneficiaries per quarter, respectively (95% CIs: -2.1 to -0.4 and -4.8 to -1.3), and hospitalizations and emergency department visits decreased in the clinically vulnerable cohort by 2.9 and 4.1 events per 1000 beneficiaries per quarter, respectively (95% CIs: -5.2 to -0.7 and -7.1 to -1.2). Changes in total spending associated with ACOs did not vary by clinical condition of beneficiaries.
Conclusions and relevance: Medicare ACO programs are associated with modest reductions in spending and use of hospitals and emergency departments. Savings were realized through reductions in use of institutional settings in clinically vulnerable patients.
Conflict of interest statement
Figures
References
-
- Muhlestein D, Gardner P, Caughey W, deLisle K. Projected Growth of Accountable Care Organizations. Leavitt Partners. http://leavittpartners.com/2015/12/projected-growth-of-accountable-care-.... Published online December 23, 2015. Accessed May 19, 2016.
-
- Nyweide DJ, Lee W, Cuerdon TT, et al. Association of Pioneer Accountable Care Organizations vs traditional Medicare fee for service with spending, utilization, and patient experience. JAMA. 2015;313(21):2152–2161. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
