

Comparing Use of Low-Value Health Care Services Among U.S. Advanced Practice Clinicians and Physicians
- PMID: 27322541
- PMCID: PMC5584613
- DOI: 10.7326/M15-2152
Comparing Use of Low-Value Health Care Services Among U.S. Advanced Practice Clinicians and Physicians
Abstract
Background: Many physicians believe that advanced practice clinicians (APCs [nurse practitioners and physician assistants]) provide care of relatively lower value.
Objective: To compare use of low-value services among U.S. APCs and physicians.
Design: Service use after primary care visits was evaluated for 3 conditions after adjustment for patient and provider characteristics and year. Patients with guideline-based red flags were excluded and analyses stratified by office- versus hospital-based visits, acute versus nonacute presentations, and whether clinicians self-identified as the patient's primary care provider (PCP).
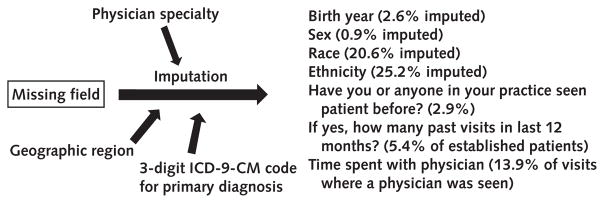
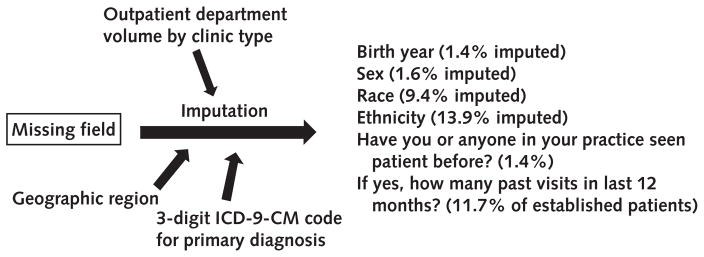
Setting: National Ambulatory Medical Care Survey (NAMCS) and National Hospital Ambulatory Medical Care Survey (NHAMCS), 1997 to 2011.
Patients: Patients presenting with upper respiratory infections (URIs), back pain, or headache.
Measurements: Use of guideline-discordant antibiotics (for URIs), radiography (for URIs and back pain), computed tomography (CT) or magnetic resonance imaging (MRI) (for headache and back pain), and referrals to other physicians (for all 3 conditions).
Results: 12 170 physician and 473 APC office-based visits and 13 359 physician and 2947 APC hospital-based visits were identified. Although office-based clinicians saw similar patients, hospital-based APCs saw younger patients (mean age, 42.6 vs. 45.0 years; P < 0.001), and practiced in urban settings less frequently (49.7% vs. 81.7% of visits; P < 0.001) than hospital-based physicians. Unadjusted and adjusted results revealed that APCs ordered antibiotics, CT or MRI, radiography, and referrals as often as physicians in both settings. Stratification suggested that self-identified PCP APCs ordered more services than PCP physicians in the hospital-based setting.
Limitation: NHAMCS reflects hospital-based APC care; NAMCS samples physician practices and likely underrepresents office-based APCs.
Conclusion: APCs and physicians provided an equivalent amount of low-value health services, dispelling physicians' perceptions that APCs provide lower-value care than physicians for these common conditions.
Primary funding source: U.S. Health Services and Research Administration, Ryoichi Sasakawa Fellowship Fund, and National Institutes of Health.
Figures
Comment in
-
Advanced Practice Clinicians and Physicians in Primary Care: Still More Questions than Answers.Ann Intern Med. 2016 Aug 16;165(4):290-1. doi: 10.7326/M16-1326. Epub 2016 Jun 21. Ann Intern Med. 2016. PMID: 27322738 No abstract available.
-
Comparing Use of Low-Value Health Care Services Among U.S. Advanced Practice Clinicians and Physicians.Ann Intern Med. 2017 Jan 3;166(1):76. doi: 10.7326/L16-0550. Ann Intern Med. 2017. PMID: 28030669 No abstract available.
-
Comparing Use of Low-Value Health Care Services Among U.S. Advanced Practice Clinicians and Physicians.Ann Intern Med. 2017 Jan 3;166(1):76. doi: 10.7326/L16-0551. Ann Intern Med. 2017. PMID: 28030670 No abstract available.
-
Comparing Use of Low-Value Health Care Services Among U.S. Advanced Practice Clinicians and Physicians.Ann Intern Med. 2017 Jan 3;166(1):77. doi: 10.7326/L16-0552. Ann Intern Med. 2017. PMID: 28030671 No abstract available.
-
Using NAMCS and NHAMCS to Examine Health Care by U.S. Physician Assistants and Nurse Practitioners.JAAPA. 2017 Feb;30(2):53. JAAPA. 2017. PMID: 31579264 Free PMC article. No abstract available.
References
-
- U.S. Department of Health and Human Services, Health Resources and Services Administration, National Center for Health Workforce Analysis. Projecting the Supply and Demand for Primary Care Practitioners Through 2020. Rockville, MD: U.S. Department of Health and Human Services; 2013. [on 20 January 2016]. Accessed at http://bhpr.hrsa.gov/healthworkforce/supplydemand/usworkforce/primarycar...
-
- Lipner RS, Bylsma WH, Arnold GK, Fortna GS, Tooker J, Cassel CK. Who is maintaining certification in internal medicine—and why? A national survey 10 years after initial certification. Ann Intern Med. 2006;144:29–36. - PubMed
Web-Only Reference
-
- McCaig LF, McLemore T. Plan and operation of the National Hospital Ambulatory Medical Survey. Series 1: programs and collection procedures. Vital Health Stat. 1994;1:1–78. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous