

Association Between Hypodensities Detected by Computed Tomography and Hematoma Expansion in Patients With Intracerebral Hemorrhage
- PMID: 27323314
- PMCID: PMC5584601
- DOI: 10.1001/jamaneurol.2016.1218
Association Between Hypodensities Detected by Computed Tomography and Hematoma Expansion in Patients With Intracerebral Hemorrhage
Abstract
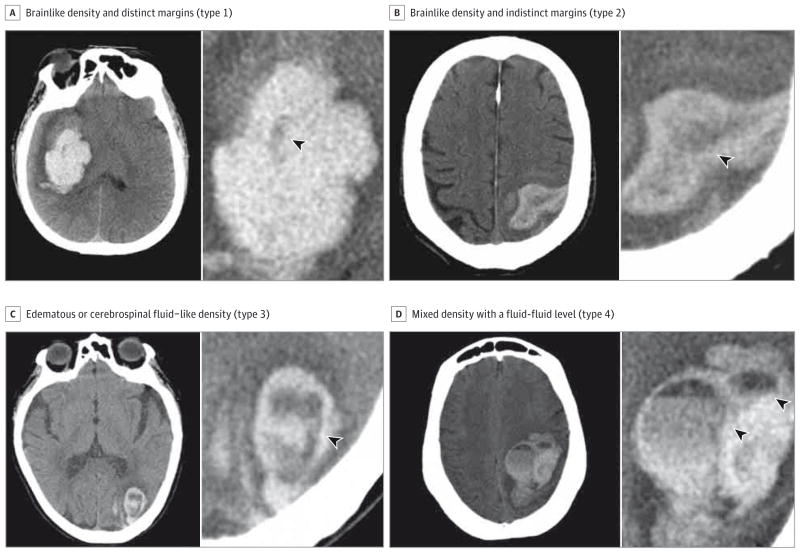
Importance: Hematoma expansion is a potentially modifiable predictor of poor outcome following an acute intracerebral hemorrhage (ICH). The ability to identify patients with ICH who are likeliest to experience hematoma expansion and therefore likeliest to benefit from expansion-targeted treatments remains an unmet need. Hypodensities within an ICH detected by noncontrast computed tomography (NCCT) have been suggested as a predictor of hematoma expansion.
Objective: To determine whether hypodense regions, irrespective of their specific patterns, are associated with hematoma expansion in patients with ICH.
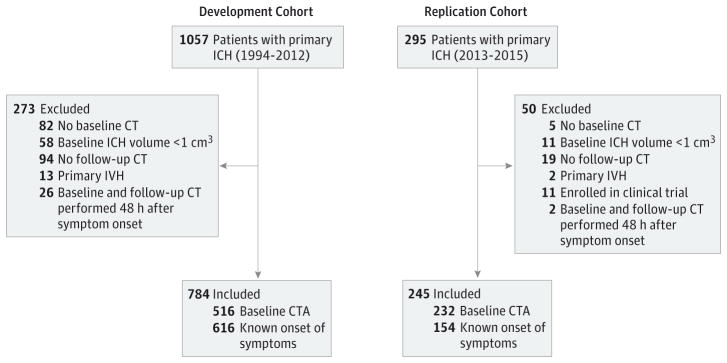
Design, setting, and participants: We analyzed a large cohort of 784 patients with ICH (the development cohort; 55.6% female), examined NCCT findings for any hypodensity, and replicated our findings on a different cohort of patients (the replication cohort; 52.7% female). Baseline and follow-up NCCT data from consecutive patients with ICH presenting to a tertiary care hospital between 1994 and 2015 were retrospectively analyzed. Data analyses were performed between December 2015 and January 2016.
Main outcomes and measures: Hypodensities were analyzed by 2 independent blinded raters. The association between hypodensities and hematoma expansion (>6 cm3 or 33% of baseline volume) was determined by multivariable logistic regression after controlling for other variables associated with hematoma expansion in univariate analyses with P ≤ .10.
Results: A total of 1029 patients were included in the analysis. In the development and replication cohorts, 222 of 784 patients (28.3%) and 99 of 245 patients (40.4%; 321 of 1029 patients [31.2%]), respectively, had NCCT scans that demonstrated hypodensities at baseline (κ = 0.87 for interrater reliability). In univariate analyses, hypodensities were associated with hematoma expansion (86 of 163 patients with hematoma expansion had hypodensities [52.8%], whereas 136 of 621 patients without hematoma expansion had hypodensities [21.9%]; P < .001). The association between hypodensities and hematoma expansion remained significant (odds ratio, 3.42 [95% CI, 2.21-5.31]; P < .001) in a multivariable model; other independent predictors of hematoma expansion were a CT angiography spot sign, a shorter time to CT, warfarin use, and older age. The independent predictive value of hypodensities was again demonstrated in the replication cohort (odds ratio, 4.37 [95% CI, 2.05-9.62]; P < .001).
Conclusion and relevance: Hypodensities within an acute ICH detected on an NCCT scan may predict hematoma expansion, independent of other clinical and imaging predictors. This novel marker may help clarify the mechanism of hematoma expansion and serve as a useful addition to clinical algorithms for determining the risk of and treatment stratification for hematoma expansion.
Conflict of interest statement
Figures
Comment in
-
Recognizing and Preventing Intracerebral Hematoma Expansion.JAMA Neurol. 2016 Aug 1;73(8):914-5. doi: 10.1001/jamaneurol.2016.1899. JAMA Neurol. 2016. PMID: 27322856 No abstract available.
References
-
- Qureshi AI, Tuhrim S, Broderick JP, Batjer HH, Hondo H, Hanley DF. Spontaneous intracerebral hemorrhage. N Engl J Med. 2001;344(19):1450–1460. - PubMed
-
- van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9(2):167–176. - PubMed
-
- Broderick JP, Brott TG, Duldner JE, Tomsick T, Huster G. Volume of intracerebral hemorrhage: a powerful and easy-to-use predictor of 30-day mortality. Stroke. 1993;24(7):987–993. - PubMed
-
- Flaherty ML, Haverbusch M, Sekar P, et al. Long-term mortality after intracerebral hemorrhage. Neurology. 2006;66(8):1182–1186. - PubMed
-
- Davis SM, Broderick J, Hennerici M, et al. Recombinant Activated Factor VII Intracerebral Hemorrhage Trial Investigators. Hematoma growth is a determinant of mortality and poor outcome after intracerebral hemorrhage. Neurology. 2006;66(8):1175–1181. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
