

Stillbirth, hypertensive disorders of pregnancy, and placental pathology
- PMID: 27324101
- PMCID: PMC5893308
- DOI: 10.1016/j.placenta.2016.04.020
Stillbirth, hypertensive disorders of pregnancy, and placental pathology
Abstract
Introduction: Stillbirth, preeclampsia, and gestational hypertension (PE/GH) have similar clinical risk factors and redundant placental pathology. We aim to discern if stillbirth with PE/GH has a particular phenotype by comparing stillbirths with and without PE/GH.
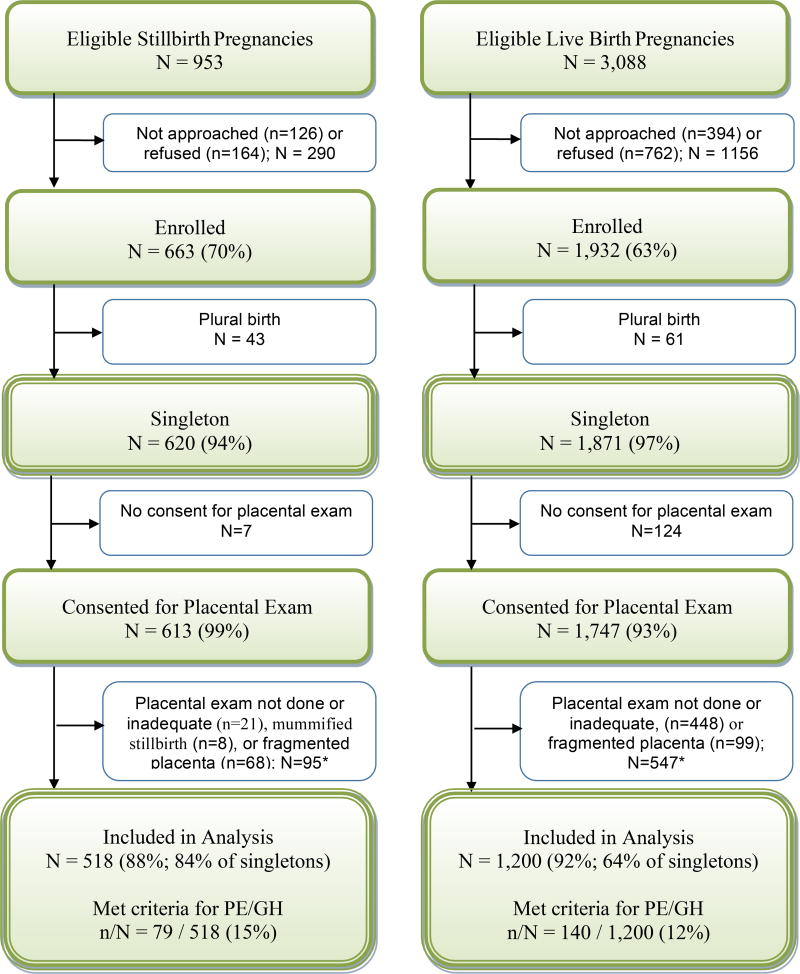
Methods: Secondary analysis of the Stillbirth Collaborative Research Network, a population-based cohort study of all stillbirths and a sample of live births from 2006 to 2008 in five catchment areas. We compared placental pathology between stillbirths and with and without PE/GH, stratified by term or preterm. We also compared placental pathology between stillbirths and live births with PE/GH.
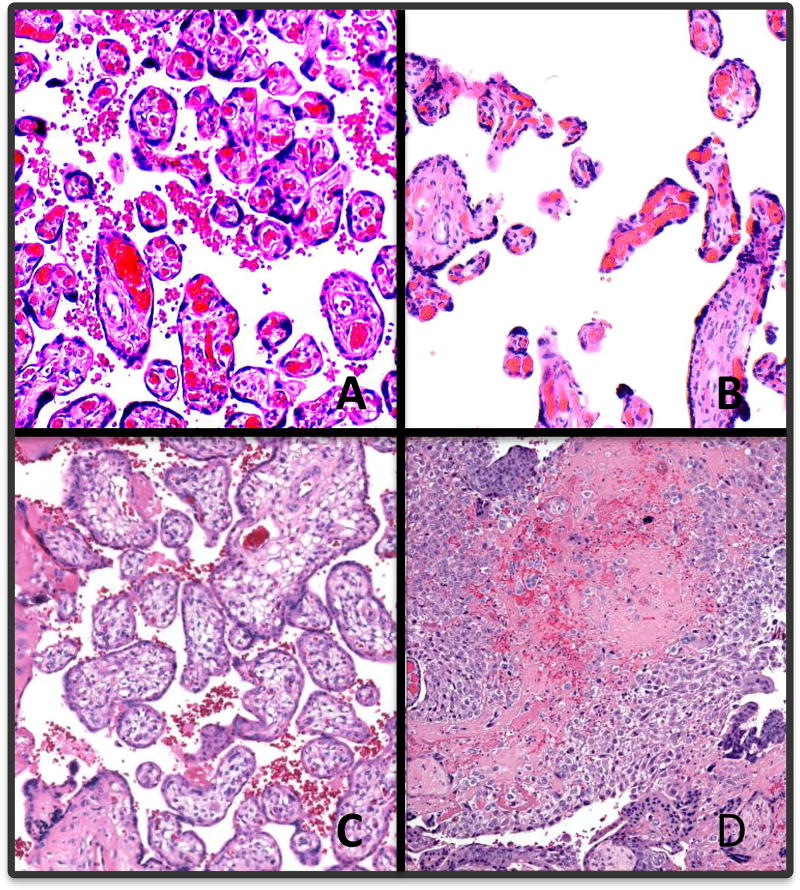
Results: 79/518 stillbirths and 140/1200 live births had PE/GH. Amongst preterm stillbirths, there was higher feto-placental ratio in PE/GH pregnancies (OR 1.24 [1.11, 1.37] per unit increase), and there were more parenchymal infarctions (OR 5.77 [3.18, 10.47]). Among PE/GH pregnancies, stillbirths had increased maternal and fetal vascular lesions, including retroplacental hematoma, parenchymal infarction, fibrin deposition, fetal vascular thrombi, and avascular villi.
Discussion: Stillbirth pregnancies are overwhelmingly associated with placental lesions. Parenchymal infarctions are more common in PE/GH preterm stillbirths, but there is significant overlap in lesions found in stillbirths and PE/GH.
Keywords: Placental pathology; Preeclampsia; Stillbirth.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
References
-
- Sibai B, Dekker G, Kupferminc M. Pre-eclampsia. Lancet. 2005;365:785–799. - PubMed
-
- Abalos E, Cuesta C, Carroli G, Qureshi Z, Widmer M, Vogel JP, et al. WHO Multicountry Survey on Maternal and Newborn Health Research Network. Pre-eclampsia, eclampsia and adverse maternal and perinatal outcomes: a secondary analysis of the World Health Organization Multicountry Survey on Maternal and Newborn Health. BJOG. 2014;121:14–24. - PubMed
-
- Haddad B, Mercer BM, Livingston JC, Sibai BM. Obstetric antecedents to apparent stillbirth (Apgar score zero at 1 minute only) Obstet Gynecol. 2001;97:961–964. - PubMed
-
- Fretts RC. Etiology and prevention of stillbirth. Am J Obstet Gynecol. 2005;193:1923–1935. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
