

Factors influencing immunologic response to hepatitis B vaccine in adults
- PMID: 27324884
- PMCID: PMC4914839
- DOI: 10.1038/srep27251
Factors influencing immunologic response to hepatitis B vaccine in adults
Abstract
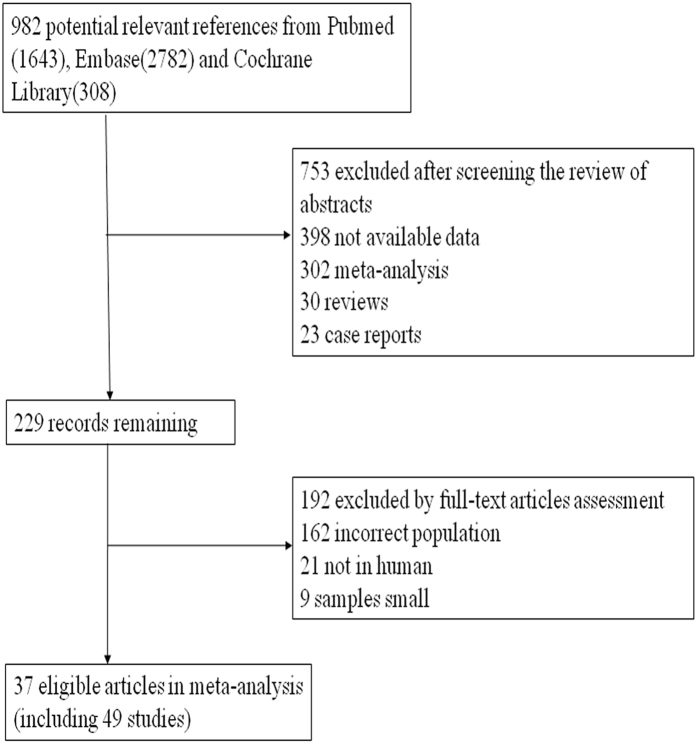
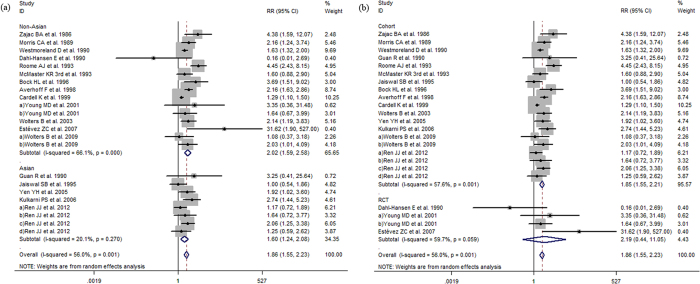
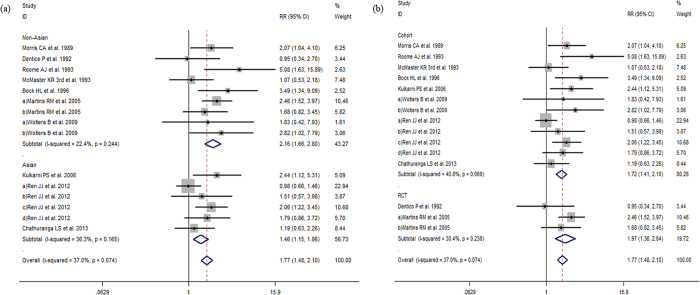
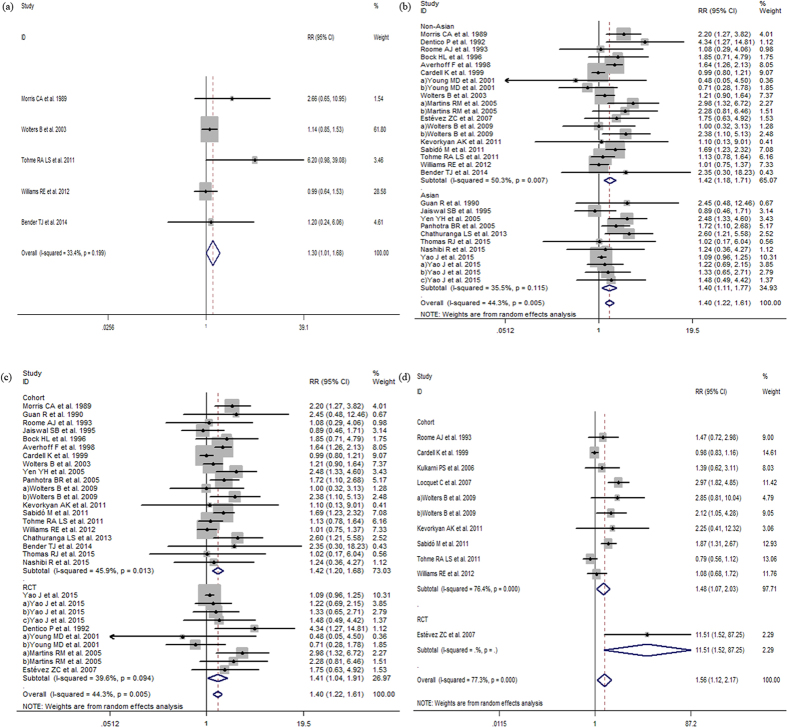
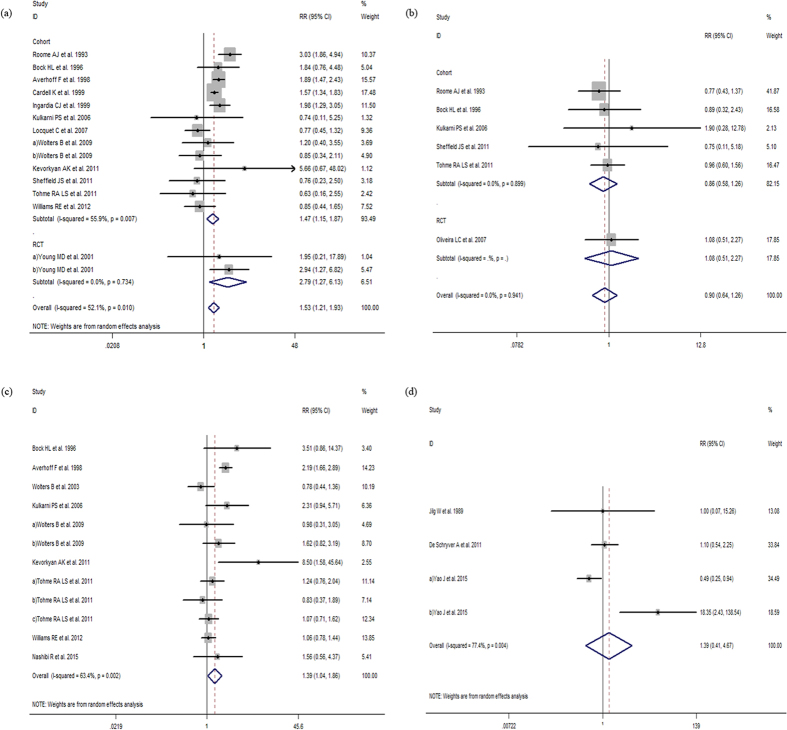
Hepatitis B was still a worldwide health problem. This study aimed to conducted a systematic review and meta-analysis to assess a more precise estimation of factors that influence the response to hepatitis B vaccine in adults. Our included studies examined seroprotection rates close to the end of vaccination schedules in healthy adult populations. This meta-analysis including 21053 adults in 37 articles showed that a significantly decreased response to hepatitis B vaccine appeared in adults (age ≥ 40) (RR:1.86, 95% CI:1.55-2.23), male adults (RR:1.40, 95% CI:1.22-1.61), BMI ≥ 25 adults (RR:1.56, 95% CI:1.12-2.17), smoker (RR:1.53, 95% CI:1.21-1.93), and adults with concomitant disease (RR:1.39, 95% CI:1.04-1.86). Meanwhile, we further found a decreased response to hepatitis B vaccine appeared in adults (age ≥ 30) (RR:1.77, 95% CI:1.48-2.10), and adults (age ≥ 60) (RR:1.30, 95% CI:1.01-1.68). However, there were no difference in response to hepatitis B vaccine both in alcoholic (RR:0.90, 95% CI:0.64-1.26) and 0-1-12 vs. 0-1-6 vaccination schedule (RR:1.39, 95% CI:0.41-4.67). Pooling of these studies recommended the sooner the better for adult hepatitis B vaccine strategy. More vaccine doses, supplemental/additional strengthening immunity should be emphasized on the susceptible population of increasing aged, male, BMI ≥ 25, smoking and concomitant disease. The conventional 0-1-6 vaccination schedule could be still worth to be recommended.
Figures
References
-
- Lavanchy D. Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. Journal of viral hepatitis 11, 97–107 (2004). - PubMed
-
- European Centre for Disease Prevention and Control. Hepatitis B and C in the EU neighbourhood: prevalence, burden of disease and screening policies. European Centre for Disease Prevention and Control. 56 p. doi: 10.2900/30933 (Stockholm, 2010). - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
