

CT findings of the temporal bone in CHARGE syndrome: aspects of importance in cochlear implant surgery
- PMID: 27324890
- PMCID: PMC5104824
- DOI: 10.1007/s00405-016-4141-z
CT findings of the temporal bone in CHARGE syndrome: aspects of importance in cochlear implant surgery
Abstract
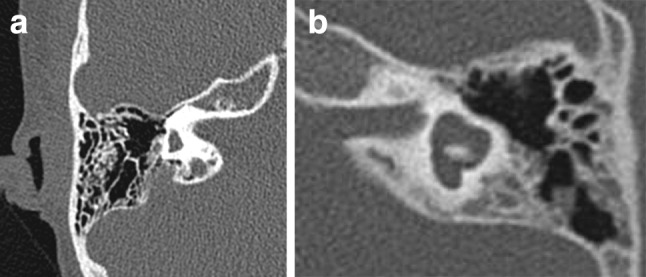
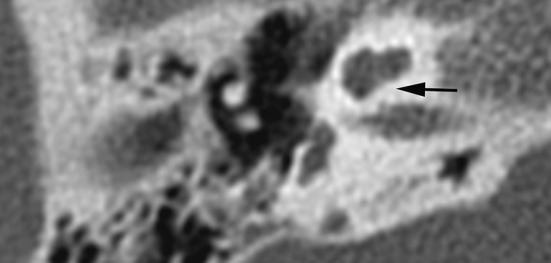
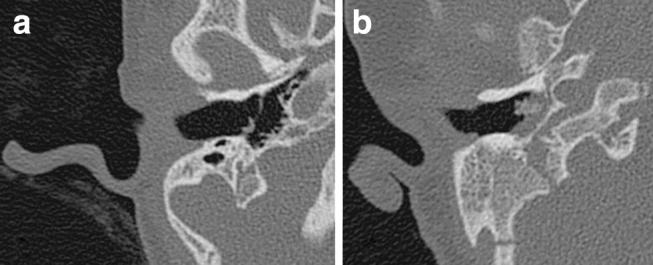
To provide an overview of anomalies of the temporal bone in CHARGE syndrome relevant to cochlear implantation (CI), anatomical structures of the temporal bone and the respective genotypes were analysed. In this retrospective study, 42 CTs of the temporal bone of 42 patients with CHARGE syndrome were reviewed in consensus by two head-and-neck radiologists and two otological surgeons. Anatomical structures of the temporal bone were evaluated and correlated with genetic data. Abnormalities that might affect CI surgery were seen, such as a vascular structure, a petrosquamosal sinus (13 %), an underdeveloped mastoid (8 %) and an aberrant course of the facial nerve crossing the round window (9 %) and/or the promontory (18 %). The appearance of the inner ear varied widely: in 77 % of patients all semicircular canals were absent and the cochlea varied from normal to hypoplastic. A stenotic cochlear aperture was observed in 37 %. The middle ear was often affected with a stenotic round (14 %) or oval window (71 %). More anomalies were observed in patients with truncating mutations than with non-truncating mutations. Temporal bone findings in CHARGE syndrome vary widely. Vascular variants, aberrant route of the facial nerve, an underdeveloped mastoid, aplasia of the semicircular canals, and stenotic round window may complicate cochlear implantation.
Keywords: Anatomy; CHARGE syndrome; Cochlear implant; Genetics; Temporal bone.
Conflict of interest statement
All authors declare that they have no conflict of interest. Ethical approval All procedures performed in the studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent Informed consent was obtained from all individual participants included in the study.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
