

Review
doi: 10.1503/cmaj.151402.
Epub 2016 Jun 20.
An overview of the diagnosis and management of immunoglobulin G4-related disease
Affiliations
- PMID: 27325130
- PMCID: PMC5026513
- DOI: 10.1503/cmaj.151402
Item in Clipboard
Review
An overview of the diagnosis and management of immunoglobulin G4-related disease
CMAJ.
.
No abstract available
Figures
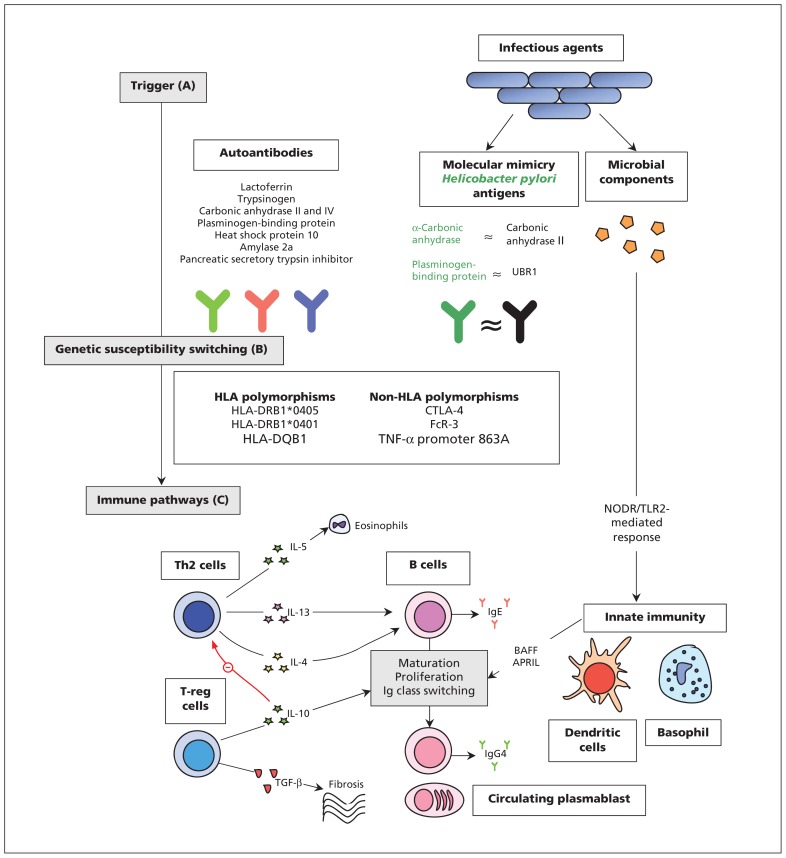
Mechanisms of pathogenesis for IgG4-related disease. (A) Antibodies versus antigens commonly found in exocrine organs may drive Th2-cell response. Most have only been investigated in type 1 AIP, are nonspecific, and none have been consistently found in active disease.– Molecular mimicry of Helicobacter pylori antigens with human counterparts may be a trigger for type 1 AIP., Microbial components may stimulate innate immune mechanisms by activating NODR and TLR2 to produce BAFF and APRIL which lead to changes to B cells in a T cell–independent manner. (B) Polymorphisms of both HLA and non-HLA antigens have been implicated in the development of type 1 AIP. (C) A dominant Th2-cell (and associated cytokine) response occurs systemically and within affected organs. An expansion in T-reg cells may contribute to both B-cell Ig class switching and fibrosis. A treatment-sensitive expansion in circulating plasmablasts is present in active disease, although their exact role in pathogenesis remains unclear. Elevated levels of IgG4 in serum is a hallmark of the disease and is a consequence of a modified Th2-cell response. Note: AIP = autoimmune pancreatitis, APRIL = a proliferation-inducing ligand, BAFF = B cell–activating factor belonging to the TNF family, B cell = beta cell, HLA = human leucocyte antigens, Ig = immunoglobulin, NODR = nucleotide-binding oligomerization domain receptor, T cell = T lymphocyte cell, TGF = transforming growth factor, Th2 = type 2 T helper, TLR2 = toll-like receptor 2, T-reg = regulatory T cell, TNF = tumour necrosis factor, UBR1 = ubiquitin-protein ligase E3 component n-recognin 1.
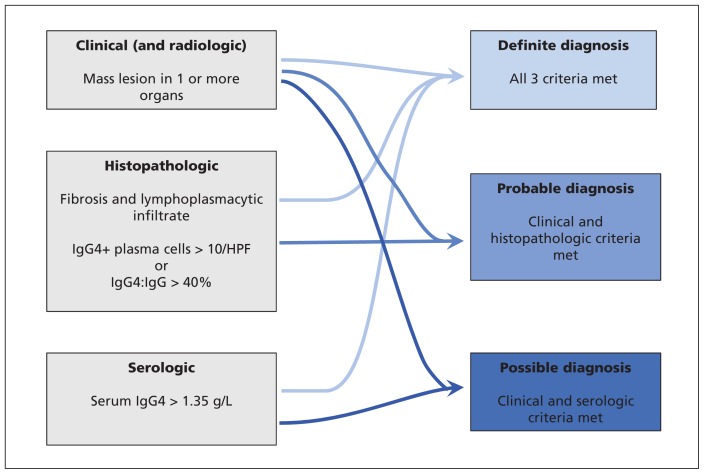
Diagnostic criteria for IgG4-related disease. HPF = high-powered field. (Adapted from Khosroshahi A, Wallace ZS, Crowe JL, et al. Arthritis Rheumatol 2015;67:1688-99).
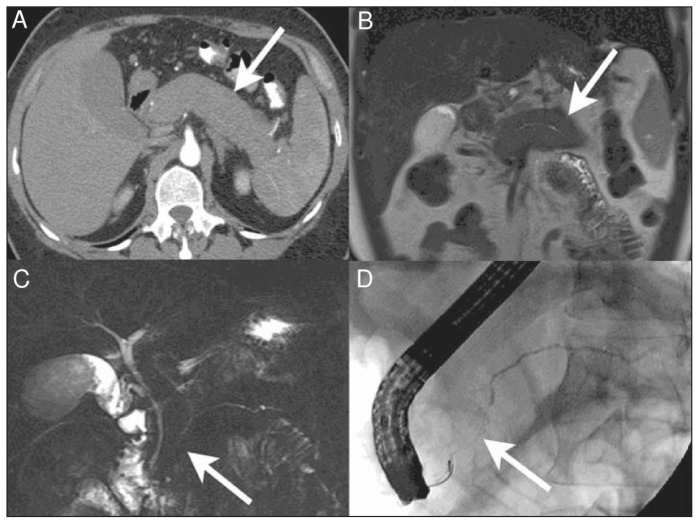
Diffuse autoimmune pancreatitis. (A) Axial computed tomography (CT) image in the pancreatic parenchymal phase of the typical enlarged and poorly enhanced pancreas in a patient with diffuse autoimmune pancreatitis (arrow). Note the lack of inflammatory change around the organ, which differentiates the disease from acute pancreatitis and necrosis. (B) View of the pancreas using coronal T2-weighted magnetic resonance imaging (MRI) that shows low signal intensity in the pancreas (arrow) because of the diffuse fibrosis in the gland. (C) Coronal magnetic resonance cholangiopancreatography image showing a diffusely irregular pancreatic duct with stenosis distally in the pancreatic head (arrow). (D) Endoscopic retrograde cholangiopancreatography image that confirms the MRI findings, including ductal stenosis (arrow). Images reproduced from reference under Creative Commons licence 2.0 (http://creativecommons.org/licenses/by/2.0/legalcode ).
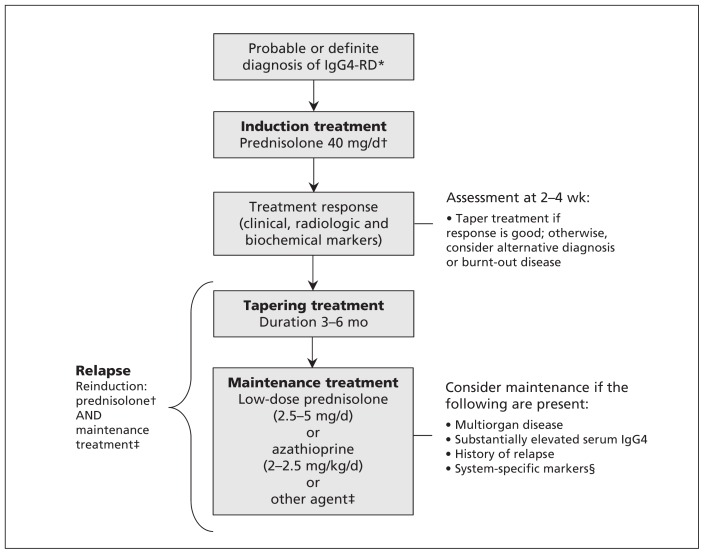
Treatment schematic for IgG4-related disease. *As diagnosed by international consensus guidance. †Consider B-cell depletion if the patient is resistant to or intolerant of glucocorticoids and therapies available to the clinician. ‡Other agents include calcineurin inhibitors, cyclophosphamide, mycophenolate mofetil and methotrexate. B-cell depletion could be considered. §Predictors of relapse in IgG4-related sclerosing cholangitis or autoimmune pancreatitis include coexisting diabetes, or a high burden of biliary involvement. Note: IgG4-RD = IgG4-related disease.
References
-
- Hamano H, Kawa S, Horiuchi A, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med 2001;344:732–8. - PubMed
-
- Kamisawa T, Funata N, Hayashi Y, et al. A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol 2003;38:982–4. - PubMed
-
- Zen Y, Harada K, Sasaki M, et al. IgG4-related sclerosing cholangitis with and without hepatic inflammatory pseudotumor, and sclerosing pancreatitis-associated sclerosing cholangitis: Do they belong to a spectrum of sclerosing pancreatitis? Am J Surg Pathol 2004;28:1193–203. - PubMed
-
- Himi T, Takano K, Yamamoto M, et al. A novel concept of Mikulicz’s disease as IgG4-related disease. Auris Nasus Larynx 2012;39:9–17. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical