

Effectiveness and Safety of Sofosbuvir-Based Regimens for Chronic HCV Genotype 3 Infection: Results of the HCV-TARGET Study
- PMID: 27325691
- PMCID: PMC4996139
- DOI: 10.1093/cid/ciw387
Effectiveness and Safety of Sofosbuvir-Based Regimens for Chronic HCV Genotype 3 Infection: Results of the HCV-TARGET Study
Abstract
Background: Sofosbuvir (SOF) is active against all hepatitis C virus (HCV) genotypes, and SOF-based therapies lead to high rates of sustained virologic response (SVR). However, genotype 3 (GT3) HCV remains a challenge with lower SVR rates reported, particularly in patients with cirrhosis. This study reports the effectiveness and safety of SOF-based therapy in patients with GT3 HCV treated in clinical practice.
Methods: Hepatitis C Virus Therapeutic Registry and Research Network is an international, prospective observational study evaluating patients treated in usual clinical practice. Patients with GT3 HCV were analyzed to assess predictors of treatment response and adverse events using descriptive statistics and multivariable logistic regression.
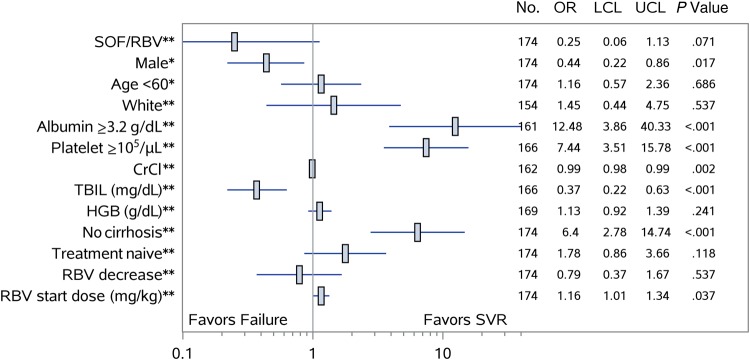
Results: Treatment outcomes were available for 197 patients treated with SOF and ribavirin (RBV), with or without peginterferon, including 54% with cirrhosis and 49% who failed prior therapy. Of 178 patients treated with SOF/RBV, 60% achieved SVR at 12 weeks (SVR12), compared with 84% of 19 patients treated with SOF/peginterferon/RBV. For patients treated with SOF/RBV, the SVR12 rate was 58% in treatment-naive patients with cirrhosis, and 42% in those with cirrhosis who failed prior therapy. In noncirrhotic patients, SVR12 rates were 89% in treatment-naive and 88% in treatment-experienced patients. After controlling for age and sex, absence of cirrhosis (odds ratio [OR], 6.4; 95% confidence interval [CI], 2.78-14.74), albumin levels ≥3.2 g/dL (OR, 12.48; 95% CI, 3.86-40.33), and platelet count >10(5) cells/µL (OR, 7.44; 95% CI, 3.51-15.78) were associated with greater odds of SVR12 CONCLUSIONS: SVR rates were acceptable in patients with GT3 HCV without cirrhosis; however, in those with cirrhosis, treatment with SOF/RBV was suboptimal, highlighting the need for new therapies for this population.
Keywords: cirrhosis; genotype 3; interferon; ribavirin; sofosbuvir.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail journals.permissions@oup.com.
Figures
References
-
- Gower E, Estes C, Blach S, Razavi-Shearer K, Razavi H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J Hepatol 2014; 61:S45–57. - PubMed
-
- Hajarizadeh B, Grebely J, Dore GJ. Epidemiology and natural history of HCV infection. Nat Rev Gastroenterol Hepatol 2013; 10:553–62. - PubMed
-
- Probst A, Dang T, Bochud M, Egger M, Negro F, Bochud PY. Role of hepatitis C virus genotype 3 in liver fibrosis progression—a systematic review and meta-analysis. J Viral Hepat 2011; 18:745–59. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
