

Ovarian Cancer Risk Factors by Histologic Subtype: An Analysis From the Ovarian Cancer Cohort Consortium
- PMID: 27325851
- PMCID: PMC5012665
- DOI: 10.1200/JCO.2016.66.8178
Ovarian Cancer Risk Factors by Histologic Subtype: An Analysis From the Ovarian Cancer Cohort Consortium
Abstract
Purpose: An understanding of the etiologic heterogeneity of ovarian cancer is important for improving prevention, early detection, and therapeutic approaches. We evaluated 14 hormonal, reproductive, and lifestyle factors by histologic subtype in the Ovarian Cancer Cohort Consortium (OC3).
Patients and methods: Among 1.3 million women from 21 studies, 5,584 invasive epithelial ovarian cancers were identified (3,378 serous, 606 endometrioid, 331 mucinous, 269 clear cell, 1,000 other). By using competing-risks Cox proportional hazards regression stratified by study and birth year and adjusted for age, parity, and oral contraceptive use, we assessed associations for all invasive cancers by histology. Heterogeneity was evaluated by likelihood ratio test.
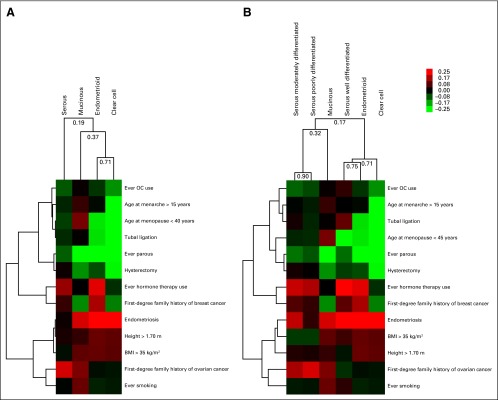
Results: Most risk factors exhibited significant heterogeneity by histology. Higher parity was most strongly associated with endometrioid (relative risk [RR] per birth, 0.78; 95% CI, 0.74 to 0.83) and clear cell (RR, 0.68; 95% CI, 0.61 to 0.76) carcinomas (P value for heterogeneity [P-het] < .001). Similarly, age at menopause, endometriosis, and tubal ligation were only associated with endometrioid and clear cell tumors (P-het ≤ .01). Family history of breast cancer (P-het = .008) had modest heterogeneity. Smoking was associated with an increased risk of mucinous (RR per 20 pack-years, 1.26; 95% CI, 1.08 to 1.46) but a decreased risk of clear cell (RR, 0.72; 95% CI, 0.55 to 0.94) tumors (P-het = .004). Unsupervised clustering by risk factors separated endometrioid, clear cell, and low-grade serous carcinomas from high-grade serous and mucinous carcinomas.
Conclusion: The heterogeneous associations of risk factors with ovarian cancer subtypes emphasize the importance of conducting etiologic studies by ovarian cancer subtypes. Most established risk factors were more strongly associated with nonserous carcinomas, which demonstrate challenges for risk prediction of serous cancers, the most fatal subtype.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at www.jco.org. Author contributions are found at the end of this article.
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386. - PubMed
-
- Buys SS, Partridge E, Black A, et al. Effect of screening on ovarian cancer mortality: The Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Randomized Controlled Trial. JAMA. 2011;305:2295–2303. - PubMed
-
- Fathalla MF. Incessant ovulation—a factor in ovarian neoplasia. Lancet. 1971;2:163. - PubMed
-
- Ness RB, Cottreau C. Possible role of ovarian epithelial inflammation in ovarian cancer. J Natl Cancer Inst. 1999;91:1459–1467. - PubMed
MeSH terms
Grants and funding
- 16491/CRUK_/Cancer Research UK/United Kingdom
- UM1 CA164973/CA/NCI NIH HHS/United States
- G1000143/MRC_/Medical Research Council/United Kingdom
- 1000143/MRC_/Medical Research Council/United Kingdom
- G0401527/MRC_/Medical Research Council/United Kingdom
- UM1 CA186107/CA/NCI NIH HHS/United States
- UM1 CA182913/CA/NCI NIH HHS/United States
- R01 CA077398/CA/NCI NIH HHS/United States
- R01 CA047988/CA/NCI NIH HHS/United States
- R01 HL080467/HL/NHLBI NIH HHS/United States
- RC1 HL099355/HL/NHLBI NIH HHS/United States
- UM1 CA182876/CA/NCI NIH HHS/United States
- Z01 ES044005/ImNIH/Intramural NIH HHS/United States
- P01 CA087969/CA/NCI NIH HHS/United States
- 14136/CRUK_/Cancer Research UK/United Kingdom
- MR/N003284/1/MRC_/Medical Research Council/United Kingdom
- R01 CA067262/CA/NCI NIH HHS/United States
- G0500300/MRC_/Medical Research Council/United Kingdom
- R01 HL043851/HL/NHLBI NIH HHS/United States
- UM1 CA176726/CA/NCI NIH HHS/United States
- K05 CA154337/CA/NCI NIH HHS/United States
- R01 CA039742/CA/NCI NIH HHS/United States
- C570/A16491/CRUK_/Cancer Research UK/United Kingdom
- 001/WHO_/World Health Organization/International
- U01 CA164973/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
