

Survival Analyses of Patients With Metastatic Renal Cancer Treated With Targeted Therapy With or Without Cytoreductive Nephrectomy: A National Cancer Data Base Study
- PMID: 27325852
- PMCID: PMC5024547
- DOI: 10.1200/JCO.2016.66.7931
Survival Analyses of Patients With Metastatic Renal Cancer Treated With Targeted Therapy With or Without Cytoreductive Nephrectomy: A National Cancer Data Base Study
Abstract
Purpose: The role of cytoreductive nephrectomy (CN) in metastatic renal cell carcinoma (mRCC) has become unclear since the introduction of targeted therapies (TT). We sought to evaluate contemporary utilization rates of CN and to examine the survival benefit of CN compared with non-CN patients treated with TT.
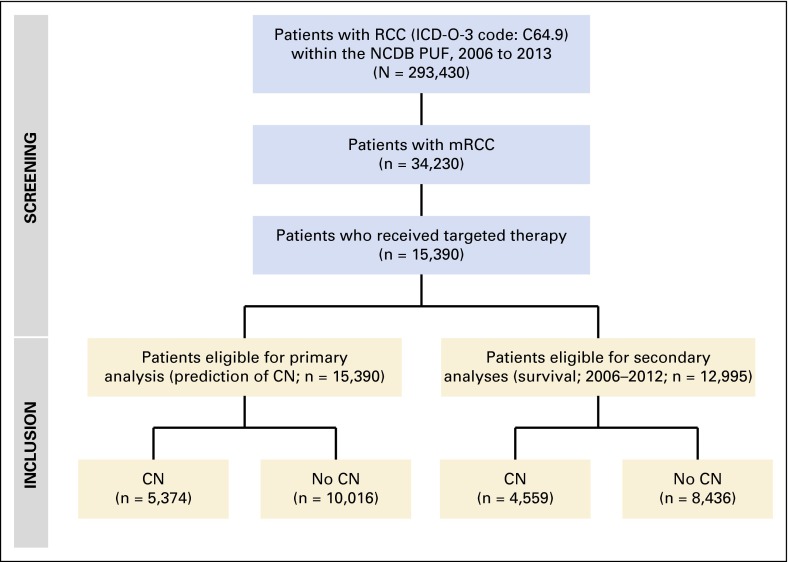
Methods: We used the National Cancer Data Base to identify patients with clinical mRCC treated with TT between 2006 and 2013. The intervention of interest was CN. Multivariable logistic regression predicting receipt of CN was performed. Overall survival (OS) was examined using Cox regression models and incremental survival analyses were performed. Sensitivity analyses using propensity scores were conducted.
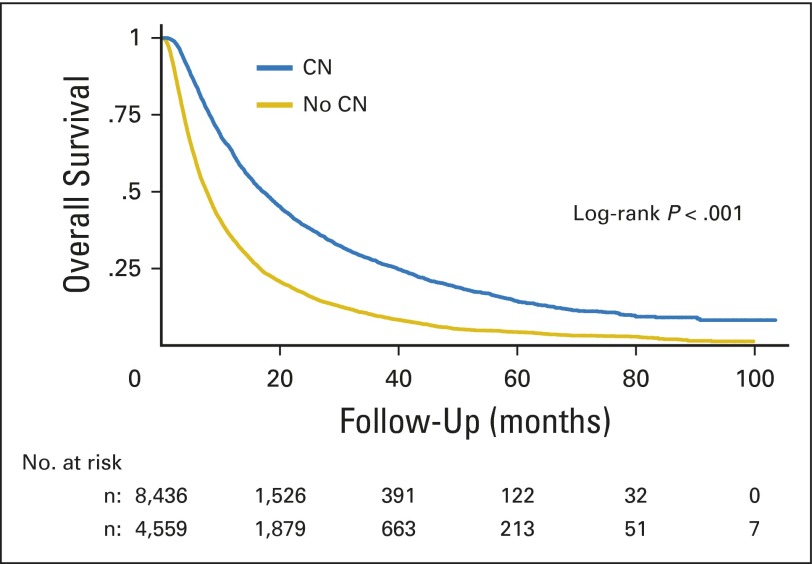
Results: Of 15,390 patients treated with TT, 5,374 (35%) underwent CN between 2006 and 2013. Patients who were younger, privately insured, treated at an academic center, and had lower tumor stage and cN0 disease were more likely to undergo CN. The median OS of CN versus non-CN patients was 17.1 (95% CI, 16.3 to 18.0 months) versus 7.7 months (95% CI, 7.4 to 7.9 months; P < .001). In sensitivity analyses using propensity scores adjustment in addition to other available covariates, CN patients had a lower risk of any death (hazard ratio, 0.45; 95% CI, 0.40 to 0.50; P < .001). The survival benefit of CN was +0.7 and +3.6 months in patients who survived ≤ 6 and ≤ 24 months, respectively, versus no CN.
Conclusion: CN is performed in three of 10 patients with mRCC who are receiving TT. Several patient and sociodemographic characteristics were associated with receipt of CN. When feasible, CN may offer an OS benefit when combined with TT.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at www.jco.org. Author contributions are found at the end of this article.
Figures
Comment in
-
Is Underutilization of Cytoreductive Nephrectomy in Patients With Metastatic Renal Cancer Contributing to Inferior Survival?J Clin Oncol. 2016 Sep 20;34(27):3235-6. doi: 10.1200/JCO.2016.68.4050. Epub 2016 Aug 15. J Clin Oncol. 2016. PMID: 27528717 No abstract available.
-
Immediate or Delayed Nephrectomy in Patients With Metastatic Renal Cancer Who Are Receiving Targeted Agents: Is the Analysis at Risk for Guarantee-Time Bias?J Clin Oncol. 2017 Apr 10;35(11):1264. doi: 10.1200/JCO.2016.69.3580. Epub 2017 Feb 6. J Clin Oncol. 2017. PMID: 28165894 No abstract available.
-
Cytoreductive Nephrectomy in Metastatic Renal Cell Carcinoma in the Era of Targeted Therapy: Scientifically Relevant or Natural Selection?J Clin Oncol. 2017 Apr 10;35(11):1265-1266. doi: 10.1200/JCO.2016.70.8156. Epub 2017 Feb 6. J Clin Oncol. 2017. PMID: 28165897 No abstract available.
-
Reply to C. Buttigliero et al and B. Biswas et al.J Clin Oncol. 2017 Apr 10;35(11):1266-1267. doi: 10.1200/JCO.2016.71.7249. Epub 2017 Feb 6. J Clin Oncol. 2017. PMID: 28165905 No abstract available.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29. - PubMed
-
- Flanigan RC, Mickisch G, Sylvester R, et al. Cytoreductive nephrectomy in patients with metastatic renal cancer: A combined analysis. J Urol. 2004;171:1071–1076. - PubMed
-
- US Food and Drug Administration: Center for Drug Evaluation and Research Approval Package for Application Number NDA 21-923. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2005/021923_s000_Nexav....
-
- Psutka SP, Kim SP, Gross CP, et al. The impact of targeted therapy on management of metastatic renal cell carcinoma: Trends in systemic therapy and cytoreductive nephrectomy utilization. Urology. 2015;85:442–451. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
