

OpenVigil FDA - Inspection of U.S. American Adverse Drug Events Pharmacovigilance Data and Novel Clinical Applications
- PMID: 27326858
- PMCID: PMC4915658
- DOI: 10.1371/journal.pone.0157753
OpenVigil FDA - Inspection of U.S. American Adverse Drug Events Pharmacovigilance Data and Novel Clinical Applications
Abstract
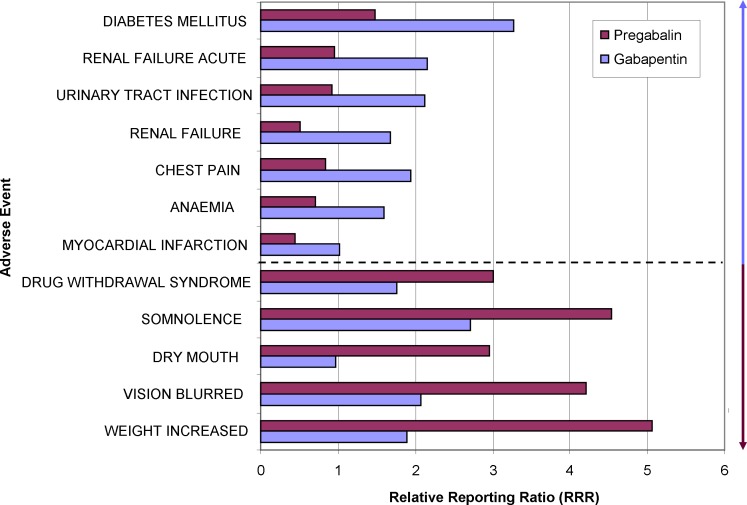
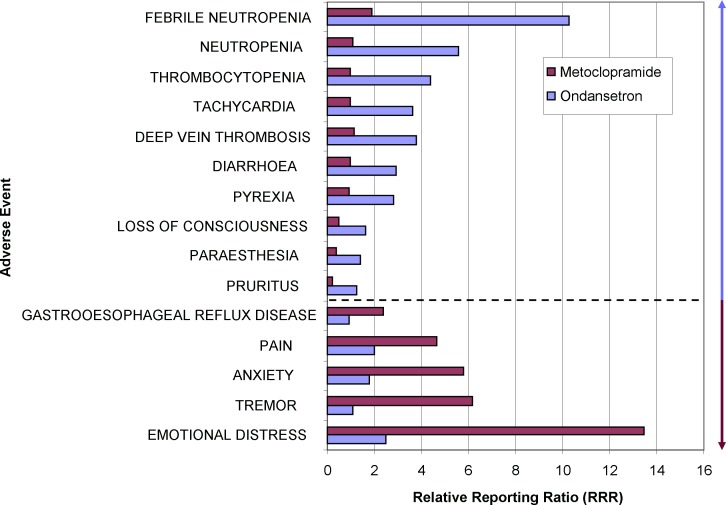
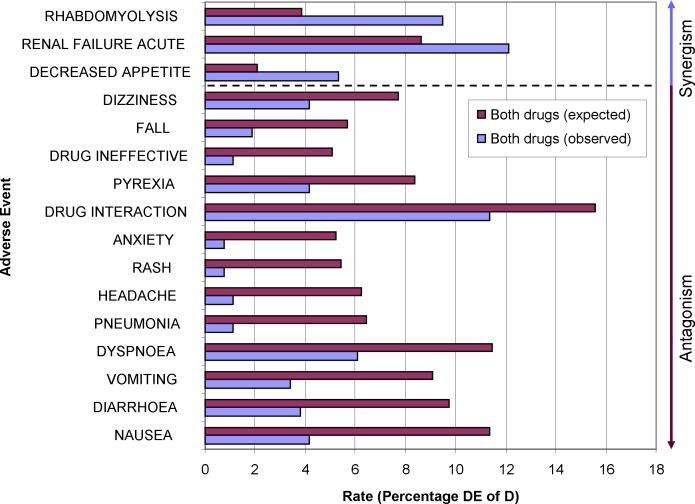
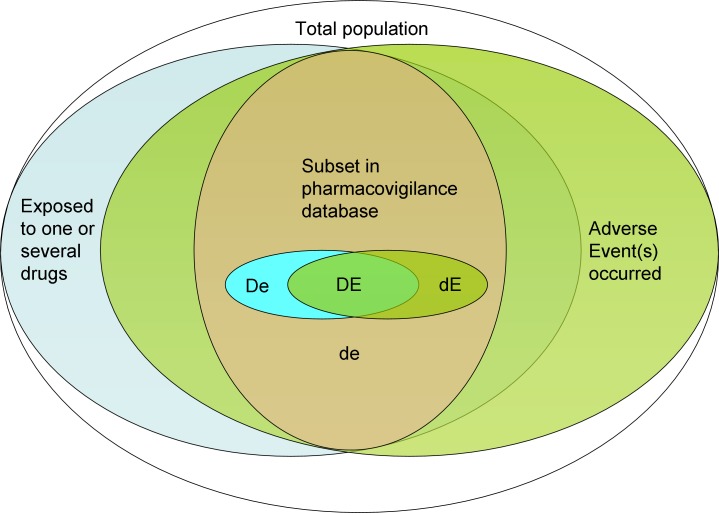
Pharmacovigilance contributes to health care. However, direct access to the underlying data for academic institutions and individual physicians or pharmacists is intricate, and easily employable analysis modes for everyday clinical situations are missing. This underlines the need for a tool to bring pharmacovigilance to the clinics. To address these issues, we have developed OpenVigil FDA, a novel web-based pharmacovigilance analysis tool which uses the openFDA online interface of the Food and Drug Administration (FDA) to access U.S. American and international pharmacovigilance data from the Adverse Event Reporting System (AERS). OpenVigil FDA provides disproportionality analyses to (i) identify the drug most likely evoking a new adverse event, (ii) compare two drugs concerning their safety profile, (iii) check arbitrary combinations of two drugs for unknown drug-drug interactions and (iv) enhance the relevance of results by identifying confounding factors and eliminating them using background correction. We present examples for these applications and discuss the promises and limits of pharmacovigilance, openFDA and OpenVigil FDA. OpenVigil FDA is the first public available tool to apply pharmacovigilance findings directly to real-life clinical problems. OpenVigil FDA does not require special licenses or statistical programs.
Conflict of interest statement
Figures
References
-
- Pitts PJ. openFDA An Open Question. Therapeutic Innovation & Regulatory Science. 2015;49(2):254–5. - PubMed
-
- Hamamoto T, Serizawa A, Ohtsuki K, Kawakami J, Sato K. [Visualization and analysis of adverse reactions of molecularly targeted anticancer agents using the self-organizing map (SOM)]. Yakugaku Zasshi. 2014;134(10):1069–80. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
