

Role of the microbiome, probiotics, and 'dysbiosis therapy' in critical illness
- PMID: 27327243
- PMCID: PMC5065053
- DOI: 10.1097/MCC.0000000000000321
Role of the microbiome, probiotics, and 'dysbiosis therapy' in critical illness
Abstract
Purpose of review: Loss of 'health-promoting' microbes and overgrowth of pathogenic bacteria (dysbiosis) in ICU is believed to contribute to nosocomial infections, sepsis, and organ failure (multiple organ dysfunction syndrome). This review discusses new understanding of ICU dysbiosis, new data for probiotics and fecal transplantation in ICU, and new data characterizing the ICU microbiome.
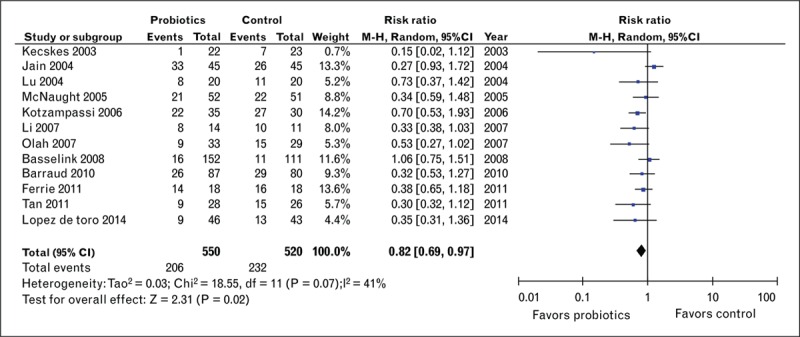
Recent findings: ICU dysbiosis results from many factors, including ubiquitous antibiotic use and overuse. Despite advances in antibiotic therapy, infections and mortality from often multidrug-resistant organisms (i.e., Clostridium difficile) are increasing. This raises the question of whether restoration of a healthy microbiome via probiotics or other 'dysbiosis therapies' would be an optimal alternative, or parallel treatment option, to antibiotics. Recent clinical data demonstrate probiotics can reduce ICU infections and probiotics or fecal microbial transplant (FMT) can treat Clostridium difficile. This contributes to recommendations that probiotics should be considered to prevent infection in ICU. Unfortunately, significant clinical variability limits the strength of current recommendations and further large clinical trials of probiotics and FMT are needed. Before larger trials of 'dysbiosis therapy' can be thoughtfully undertaken, further characterization of ICU dysbiosis is needed. To addressing this, we conducted an initial analysis demonstrating a rapid and marked change from a 'healthy' microbiome to an often pathogen-dominant microbiota (dysbiosis) in a broad ICU population.
Summary: A growing body of evidence suggests critical illness and ubiquitous antibiotic use leads to ICU dysbiosis that is associated with increased ICU infection, sepsis, and multiple organ dysfunction syndrome. Probiotics and FMT show promise as ICU therapies for infection. We hope future-targeted therapies using microbiome signatures can be developed to correct 'illness-promoting' dysbiosis to restore a healthy microbiome post-ICU to improve patient outcomes.
Figures


References
-
- Vincent JL, Rello J, Marshall J, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009; 302:2323–2329. - PubMed
-
- Ruttimann S, Keck B, Hartmeier C, et al. Long-term antibiotic cost savings from a comprehensive intervention program in a medical department of a university-affiliated teaching hospital. Clin Infect Dis 2004; 38:348–356. - PubMed
-
- Fridkin S, Baggs J, Fagan R, et al. Vital signs: improving antibiotic use among hospitalized patients. MMWR Morb Mortal Wkly Rep 2014; 63:194–200. - PMC - PubMed
-
The key report evaluates antibiotic prescribing practice in 183 US hospitals and shows antibiotic prescribing could be improved in 37.2% of the most common prescription scenarios reviewed. Further, they estimate if a 30% reduction in use of broad-spectrum antibiotics (would reduce overall antibiotic use by only 5%) could be achieved this would prevent 26% of C. difficile infections related to inpatient antibiotic use. Overall, evidence of incorrect prescribing and observed variability in current usage patterns suggest that improvements are needed and will benefit patients.
-
- Lessa FC, Mu Y, Bamberg WM, et al. Burden of Clostridium difficile infection in the United States. N Engl J Med 2015; 372:825–834. - PMC - PubMed
-
Key report of active population and laboratory-based surveillance across 10 geographic areas in the United States in 2011 to identify cases of C. difficile infection. Results showed that C. difficile was responsible for almost half a million infections and was associated with approximately 29 000 deaths in 2011. (Funded by the Centers for Disease Control and Prevention.)
