

The myths and physiology surrounding intrapartum decelerations: the critical role of the peripheral chemoreflex
- PMID: 27328617
- PMCID: PMC5009777
- DOI: 10.1113/JP271205
The myths and physiology surrounding intrapartum decelerations: the critical role of the peripheral chemoreflex
Abstract
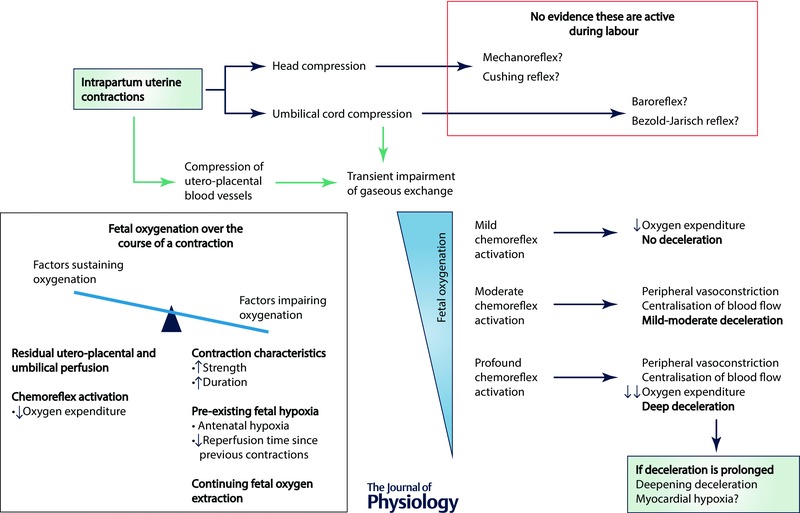
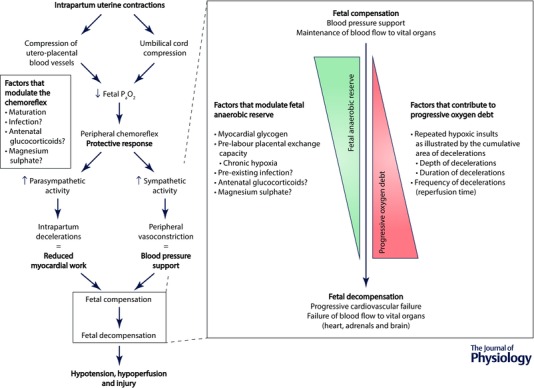
A distinctive pattern of recurrent rapid falls in fetal heart rate, called decelerations, are commonly associated with uterine contractions during labour. These brief decelerations are mediated by vagal activation. The reflex triggering this vagal response has been variably attributed to a mechanoreceptor response to fetal head compression, to baroreflex activation following increased blood pressure during umbilical cord compression, and/or a Bezold-Jarisch reflex response to reduced venous return from the placenta. Although these complex explanations are still widespread today, there is no consistent evidence that they are common during labour. Instead, the only mechanism that has been systematically investigated, proven to be reliably active during labour and, crucially, capable of producing rapid decelerations is the peripheral chemoreflex. The peripheral chemoreflex is triggered by transient periods of asphyxia that are a normal phenomenon associated with all uterine contractions. This should not cause concern as the healthy fetus has a remarkable ability to adapt to these repeated but short periods of asphyxia. This means that the healthy fetus is typically not at risk of hypotension and injury during uncomplicated labour even during repeated brief decelerations. The physiologically incorrect theories surrounding decelerations that ignore the natural occurrence of repeated asphyxia probably gained widespread support to help explain why many babies are born healthy despite repeated decelerations during labour. We propose that a unified and physiological understanding of intrapartum decelerations that accepts the true nature of labour is critical to improve interpretation of intrapartum fetal heart rate patterns.
© 2016 The Authors. The Journal of Physiology © 2016 The Physiological Society.
Figures
Comment in
-
Labouring on decelerations: the fetal peripheral chemoreflex wins.J Physiol. 2016 Sep 1;594(17):4699-700. doi: 10.1113/JP272339. J Physiol. 2016. PMID: 27581562 Free PMC article. No abstract available.
-
Is the hypothesis that the commonest fetal heart rate decelerations are caused by peripheral chemoreflex due to fetal hypoxaemia correct?J Physiol. 2017 Sep 1;595(17):6077-6080. doi: 10.1113/JP274478. J Physiol. 2017. PMID: 28856753 Free PMC article. No abstract available.
-
Reply from Christopher A. Lear, Robert Galinsky, Guido Wassink, Kyohei Yamaguchi, Joanne O. Davidson, Jenny A. Westgate, Laura Bennet and Alistair J. Gunn.J Physiol. 2017 Sep 1;595(17):6081-6083. doi: 10.1113/JP274800. J Physiol. 2017. PMID: 28856754 Free PMC article. No abstract available.
References
-
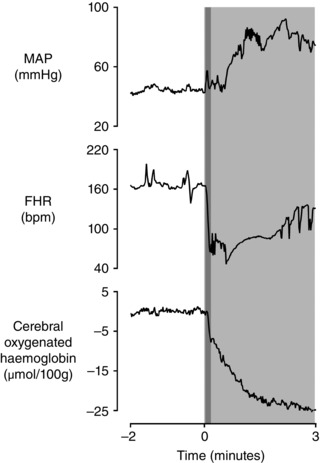
- Aldrich CJ, D'Antona D, Spencer JA, Delpy DT, Reynolds EO & Wyatt JS (1996). Fetal heart rate changes and cerebral oxygenation measured by near‐infrared spectroscopy during the first stage of labour. Eur J Obstet Gynecol Reprod Biol 64, 189–195. - PubMed
-
- Assali NS, Dasgupta K, Kolin A & Holms L (1958). Measurement of uterine blood flow and uterine metabolism. V. Changes during spontaneous and induced labor in unanesthetized pregnant sheep and dogs. Am J Physiol 195, 614–620. - PubMed
-
- Baan J Jr, Boekkooi PF, Teitel DF & Rudolph AM (1993). Heart rate fall during acute hypoxemia: a measure of chemoreceptor response in fetal sheep. J Dev Physiol 19, 105–111. - PubMed
-
- Ball RH & Parer JT (1992). The physiologic mechanisms of variable decelerations. Am J Obstet Gynecol 166, 1683–1688. - PubMed
-
- Barcroft J (1946). Researches on Pre‐natal Life. Blackwell Scientific Publications Ltd, London and Oxford.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical