

Iatrogenic hemobilia: imaging features and management with transcatheter arterial embolization in 30 patients
- PMID: 27328719
- PMCID: PMC4956024
- DOI: 10.5152/dir.2016.15295
Iatrogenic hemobilia: imaging features and management with transcatheter arterial embolization in 30 patients
Abstract
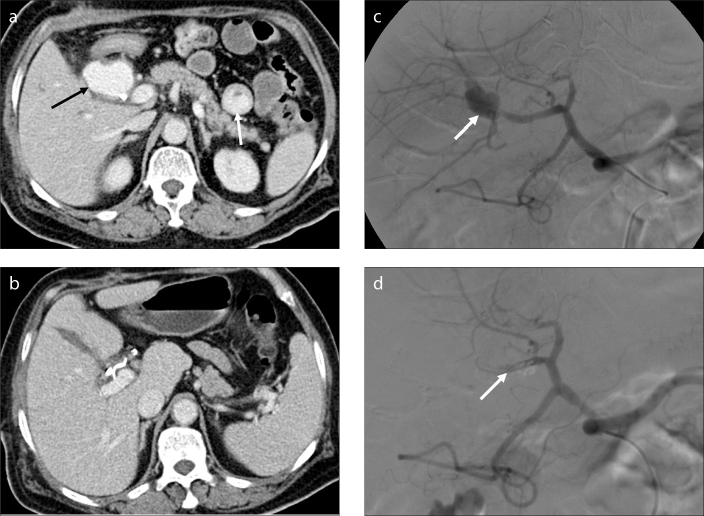
Purpose: We aimed to evaluate the imaging features of computed tomography (CT) and angiography and the efficacy of transcatheter arterial embolization (TAE) in patients with hemobilia of different iatrogenic causes.
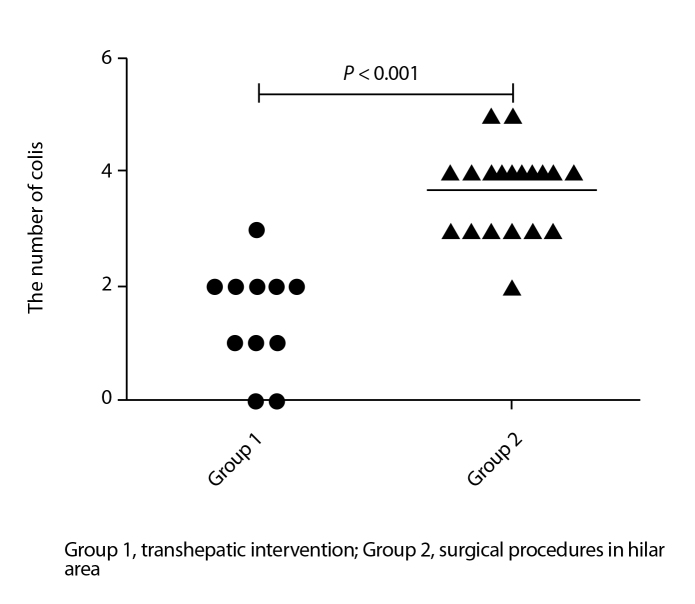
Methods: Thirty patients with hemobilia were divided into two groups according to their iatrogenic causes, i.e., group 1, 11 patients (36.7%) with transhepatic intervention and group 2, 19 patients (63.3%) with surgical procedures in the hilar area. Seventeen patients (56.7%) underwent abdominal contrast-enhanced CT before selective angiography. Polyvinyl alcohol particles, gelatin sponges, and coils were used for TAE. Data from the two groups were compared using Fisher's exact test and the Mann-Whitney U test.
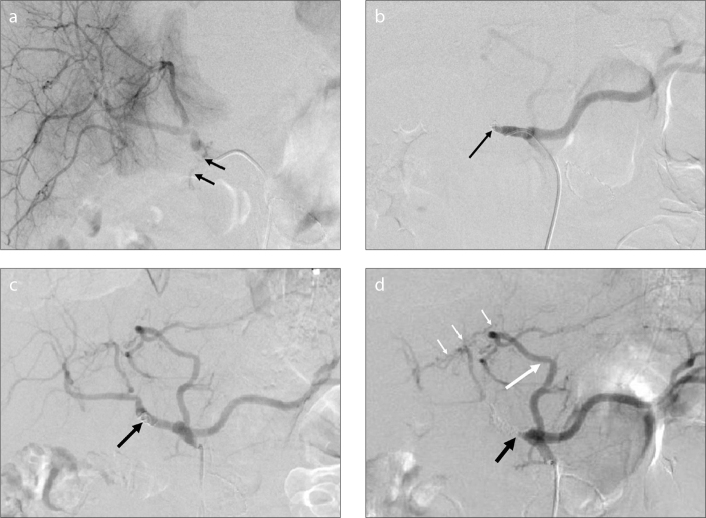
Results: Contrast-enhanced CT showed a hematoma, extravasation of contrast material, and pseudoaneurysm. The bleeding source was determined by angiographic features in all patients, which were not significantly different between the two groups (P = 0.127), and pseudoaneurysm was the most common. The embolic material and number of coils used for TAE were significantly different between the two groups (P < 0.001), but the embolization was technically successful in all patients. The clinical success rate of the first embolization was 100% in group 1 vs. 84.2% in group 2. The overall clinical success rate of TAE was 100% in all patients. The complication rate was 63.6% in group 1 vs. 68.4% in group 2 (P = 1.000).
Conclusion: CT was useful in diagnosing hemobilia, and angiograms enabled determination of the bleeding source. Pseudoaneurysm was one of the most common angiographic features. TAE was successfully performed with different embolic materials on the basis of the iatrogenic cause and bleeding location.
Figures


References
-
- Bloechle C, Izbicki JR, Rashed MY, et al. Hemobilia: presentation, diagnosis, and management. Am J Gastroenterol. 1994;89:1537–1540. - PubMed
-
- Murugesan SD, Sathyanesan J, Lakshmanan A, et al. Massive hemobilia: a diagnostic and therapeutic challenge. World J Surgery. 2014;38:1755–1762. http://dx.doi.org/10.1007/s00268-013-2435-5. - DOI - PubMed
-
- Green MHA, Johnson CD, Jamieson NV. Haemobilia. Br J Surg. 2001;88:773–786. http://dx.doi.org/10.1046/j.1365-2168.2001.01756.x. - DOI - PubMed
-
- Yoshida J, Donahue PE, Nyhus LM, et al. Hemobilia: review of recent experience with a worldwide problem. Am J Gastroenterol. 1987;82:448–453. - PubMed
-
- Cao H, Liu J, Li T, et al. Interventional therapy for the treatment of severe hemobilia after percutaneous transhepatic cholangial drainage: a case series. International Surg. 2013;98:223–228. http://dx.doi.org/10.9738/INTSURG-D-13-CC194. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
