

Orthostatic tremor: a cerebellar pathology?
- PMID: 27329770
- PMCID: PMC4958903
- DOI: 10.1093/brain/aww140
Orthostatic tremor: a cerebellar pathology?
Abstract
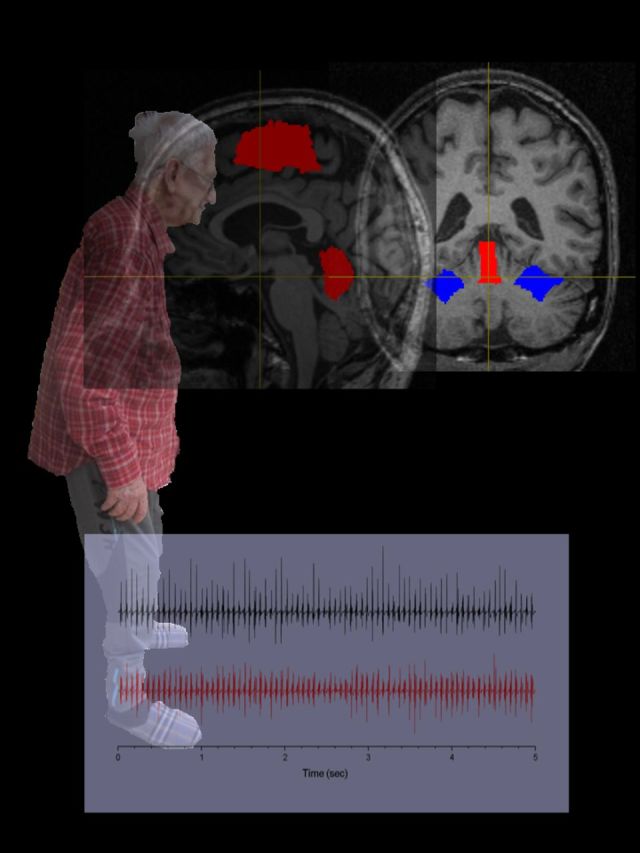
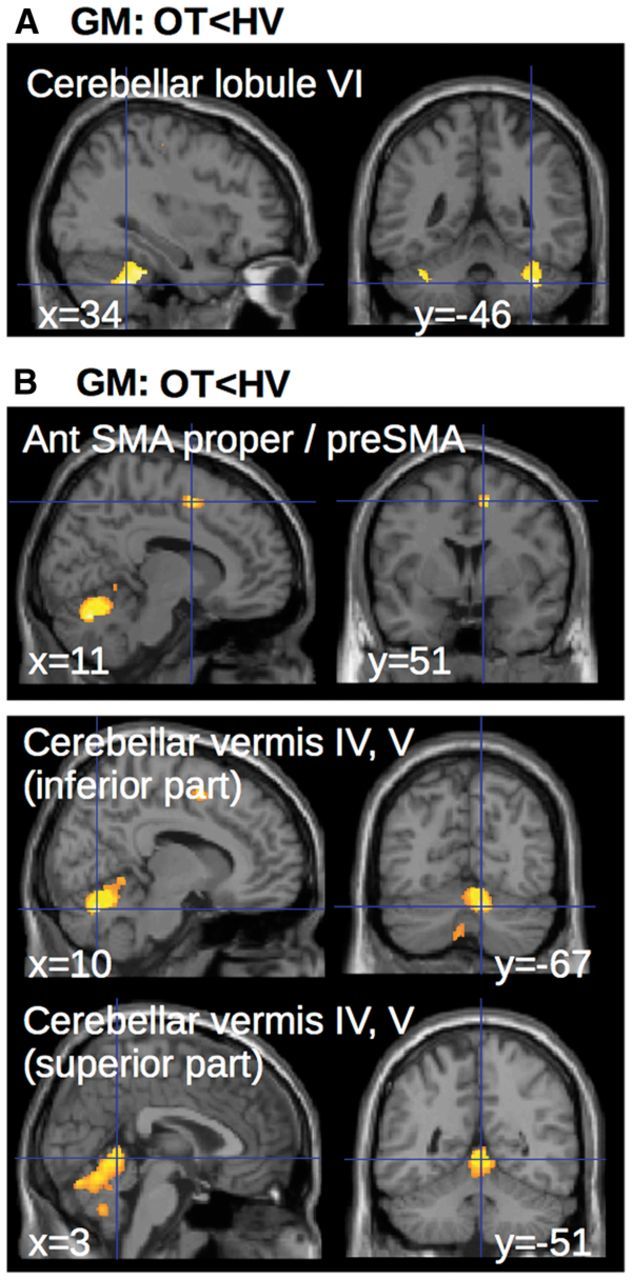
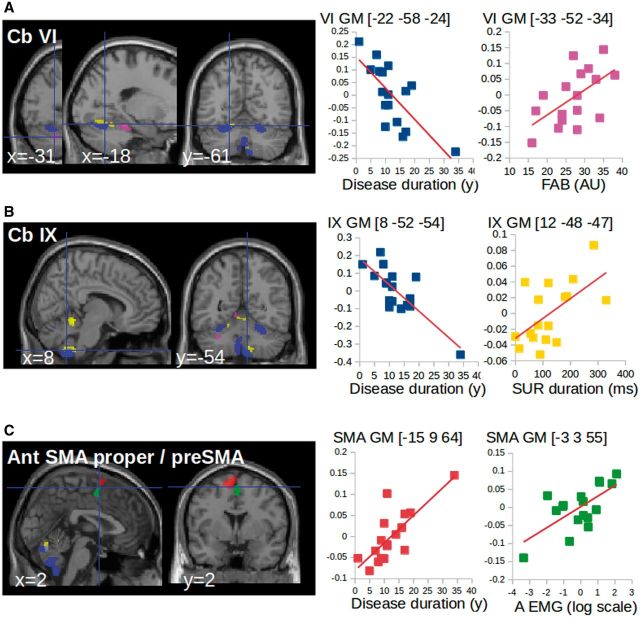
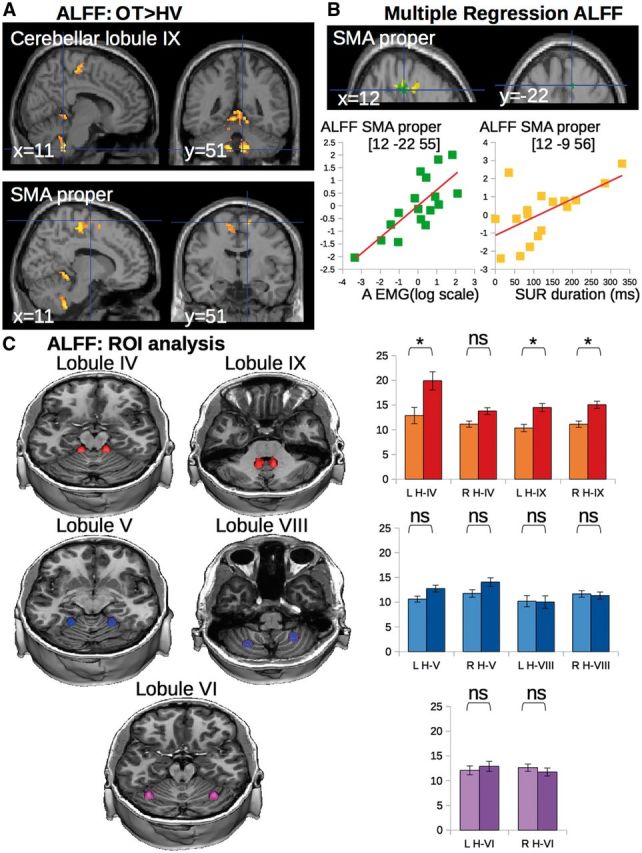
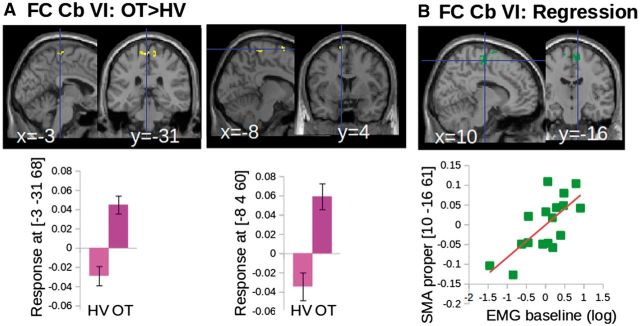
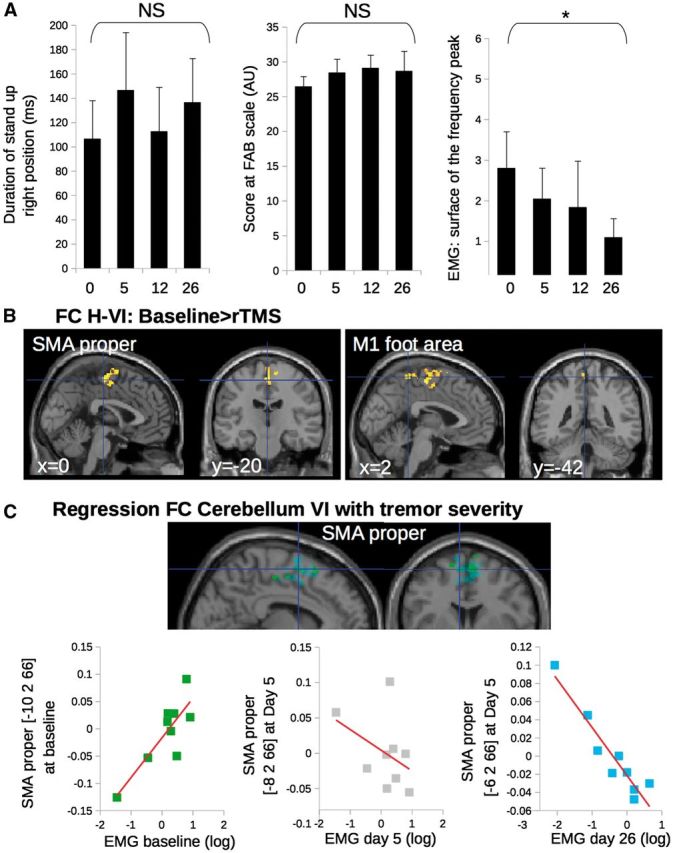
SEE MUTHURAMAN ET AL DOI101093/AWW164 FOR A SCIENTIFIC COMMENTARY ON THIS ARTICLE: Primary orthostatic tremor is characterized by high frequency tremor affecting the legs and trunk during the standing position. Cerebellar defects were suggested in orthostatic tremor without direct evidence. We aimed to characterize the anatomo-functional defects of the cerebellar motor pathways in orthostatic tremor. We used multimodal neuroimaging to compare 17 patients with orthostatic tremor and 17 age- and gender-matched healthy volunteers. Nine of the patients with orthostatic tremor underwent repetitive transcranial stimulation applied over the cerebellum during five consecutive days. We quantified the duration of standing position and tremor severity through electromyographic recordings. Compared to healthy volunteers, grey matter volume in patients with orthostatic tremor was (i) increased in the cerebellar vermis and correlated positively with the duration of the standing position; and (ii) increased in the supplementary motor area and decreased in the lateral cerebellum, which both correlated with the disease duration. Functional connectivity between the lateral cerebellum and the supplementary motor area was abnormally increased in patients with orthostatic tremor, and correlated positively with tremor severity. After repetitive transcranial stimulation, tremor severity and functional connectivity between the lateral cerebellum and the supplementary motor area were reduced. We provide an explanation for orthostatic tremor pathophysiology, and demonstrate the functional relevance of cerebello-thalamo-cortical connections in tremor related to cerebellar defects.
Keywords: cerebellar function; frontal lobe; motor cortex; movement disorder; tremor.
© The Author (2016). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Cerebello-cortical networks in orthostatic tremor.Brain. 2016 Aug;139(Pt 8):2104-6. doi: 10.1093/brain/aww164. Brain. 2016. PMID: 27457226 No abstract available.
References
-
- Asanuma C,Thach WT,Jones EG. Distribution of cerebellar terminations and their relation to other afferent terminations in the ventral lateral thalamic region of the monkey. Brain Res 1983; 286: 237–65. - PubMed
-
- Ashburner J,Friston KJ. Unified segmentation. Neuroimage 2005; 26: 839–51. - PubMed
-
- Bardinet E,Bhattacharjee M,Dormont D,Pidoux B,Malandain G,Schüpbach M,et al. . A three-dimensional histological atlas of the human basal ganglia. II. Atlas deformation strategy and evaluation in deep brain stimulation for Parkinson disease. J Neurosurg 2009; 110: 208–19. - PubMed
-
- Benito-León J,Rodríguez J,Ortí-Pareja M,Ayuso-Peralta L,Jiménez-Jiménez FJ,Molina JA. Symptomatic orthostatic tremor in pontine lesions. Neurology 1997; 49: 1439–41. - PubMed
-
- Biswal B,Yetkin FZ,Haughton VM,Hyde JS. Functional connectivity in the motor cortex of resting human brain using echo-planar MRI. Magn Reson Med 1995; 34: 537–41. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
