

Should Restrictions Be Relaxed for Metformin Use in Chronic Kidney Disease? No, We Should Never Again Compromise Safety!
- PMID: 27330129
- PMCID: PMC4915554
- DOI: 10.2337/dc15-2327
Should Restrictions Be Relaxed for Metformin Use in Chronic Kidney Disease? No, We Should Never Again Compromise Safety!
Abstract
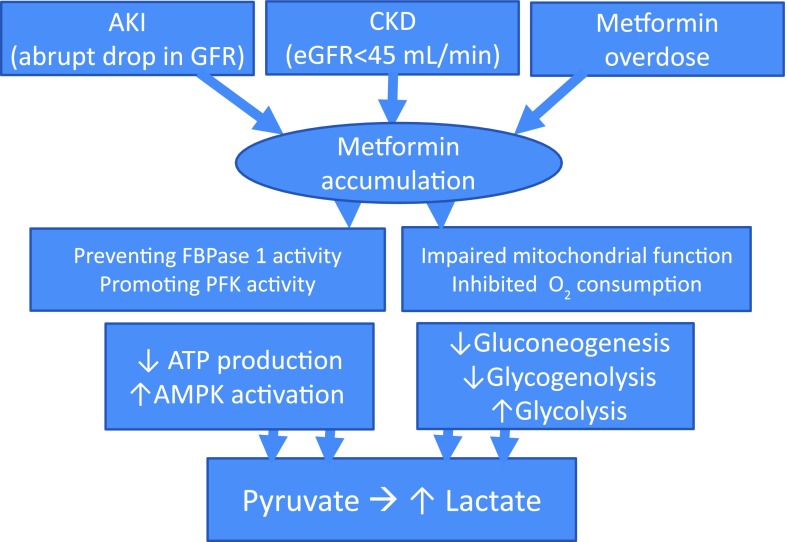
Metformin is and has been considered as first-line therapy for type 2 diabetes for over a quarter of a century. Like other biguanides, metformin can cause a lactic acidosis that is exceptionally rare but fatal. The likelihood of metformin-associated lactic acidosis is substantially higher in patients with kidney impairment and also among those with seemingly normal kidney function who are at risk of acute kidney injury (AKI). Hence, regulatory agencies in many industrialized nations have maintained strict renal restrictions surrounding metformin. However, there have been millions of people exposed to metformin for many years, many of them with serum creatinine values at or close to 1.5 mg/dL with estimated glomerular filtration rates (eGFRs) much below 60 mL/min/1.73 m(2) who have not developed lactic acidosis. Thus, there clearly remains controversy in this area, and there has been heightened pressure to remove the renal restrictions of metformin. To provide a discussion on the pros and cons of relaxing the renal restrictions for metformin use, we provide a Point-Counterpoint. In the point narrative below, Drs. Kalantar-Zadeh and Kovesdy provide their argument that although there is little evidence of the potential benefits of metformin in kidney disease, just considering the sheer numbers of metformin users and the high fatality rate of its associated lactic acidosis, the most appropriate practice is to avoid metformin use in people with eGFR <45 mL/min/1.73 m(2) or in those who are at high risk of AKI irrespective of underlying eGFR. In the following counterpoint narrative, Drs. Bakris and Molitch argue that the data from a very large analysis demonstrate clearly that serum creatinine should be supplanted with eGFR as the criteria for metformin use and that the incidence of lactic acidosis is only elevated in those with a reduced eGFR who become dehydrated for various reasons or in those exposed to some toxin resulting in AKI. Otherwise the data clearly support the use of metformin under normal circumstances down to eGFR >30 mL/min/1.73 m(2)-William T. CefaluEditor in Chief, Diabetes Care.
© 2016 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures
References
-
- Fimognari FL, Corsonello A, Pastorell R, Antonelli-Incalzi R. Metformin-induced pancreatitis: A possible adverse drug effect during acute renal failure. Diabetes Care 2006;29:1183 - PubMed
-
- Kalantar-Zadeh K, Uppot RN, Lewandrowski KB. Case records of the Massachusetts General Hospital. Case 23-2013. A 54-year-old woman with abdominal pain, vomiting, and confusion. N Engl J Med 2013;369:374–382 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
