

MIND Demons for MR-to-CT Deformable Image Registration In Image-Guided Spine Surgery
- PMID: 27330239
- PMCID: PMC4909372
- DOI: 10.1117/12.2208621
MIND Demons for MR-to-CT Deformable Image Registration In Image-Guided Spine Surgery
Abstract
Purpose: Localization of target anatomy and critical structures defined in preoperative MR images can be achieved by means of multi-modality deformable registration to intraoperative CT. We propose a symmetric diffeomorphic deformable registration algorithm incorporating a modality independent neighborhood descriptor (MIND) and a robust Huber metric for MR-to-CT registration.
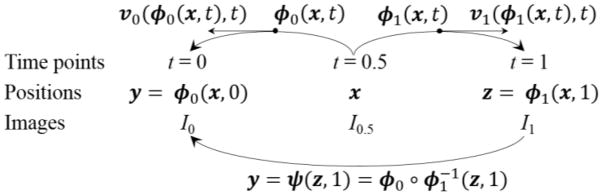
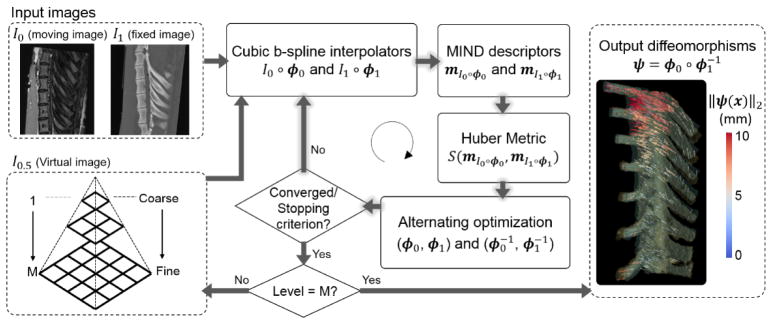
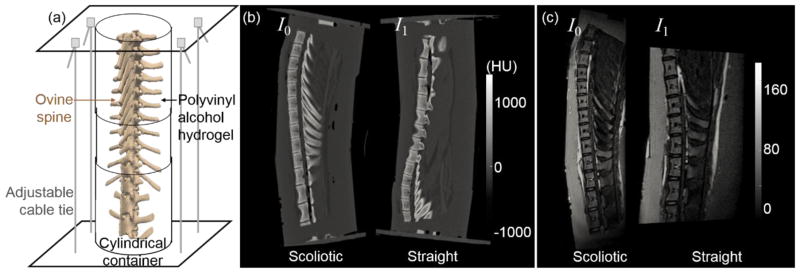
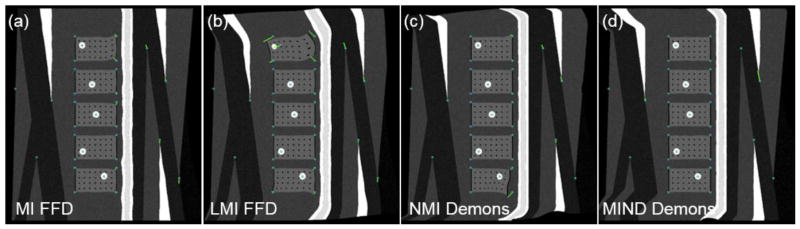
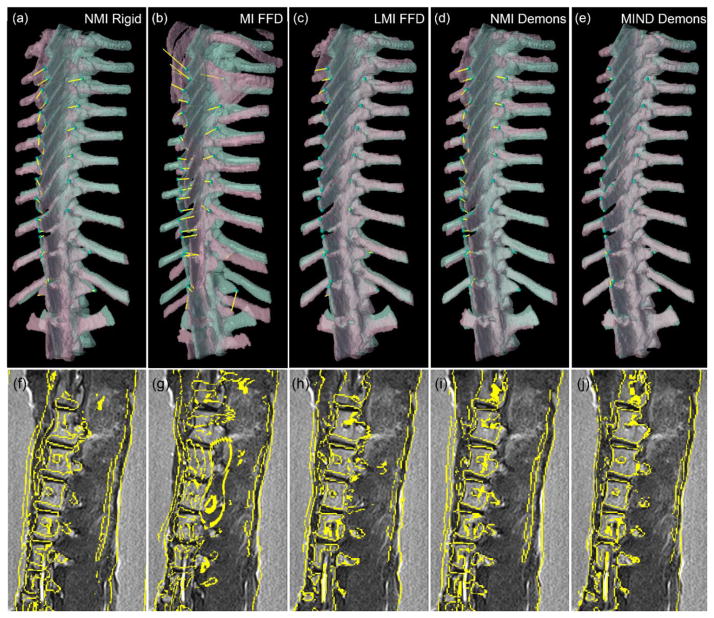
Method: The method, called MIND Demons, solves for the deformation field between two images by optimizing an energy functional that incorporates both the forward and inverse deformations, smoothness on the velocity fields and the diffeomorphisms, a modality-insensitive similarity function suitable to multi-modality images, and constraints on geodesics in Lagrangian coordinates. Direct optimization (without relying on an exponential map of stationary velocity fields used in conventional diffeomorphic Demons) is carried out using a Gauss-Newton method for fast convergence. Registration performance and sensitivity to registration parameters were analyzed in simulation, in phantom experiments, and clinical studies emulating application in image-guided spine surgery, and results were compared to conventional mutual information (MI) free-form deformation (FFD), local MI (LMI) FFD, and normalized MI (NMI) Demons.
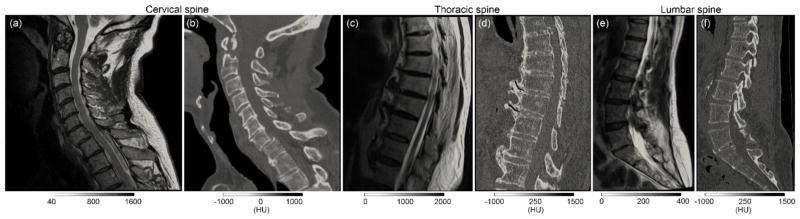
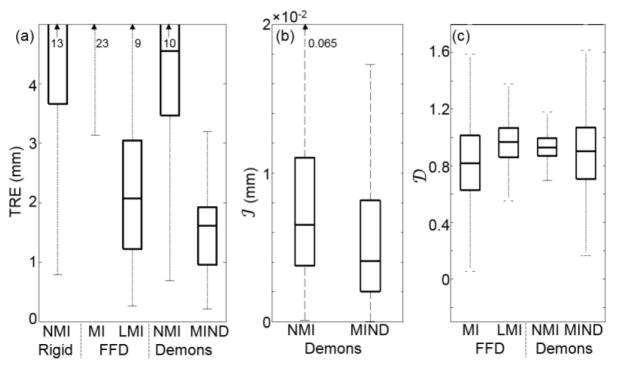
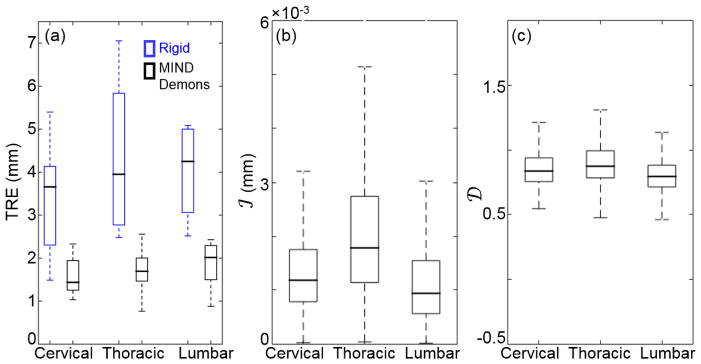
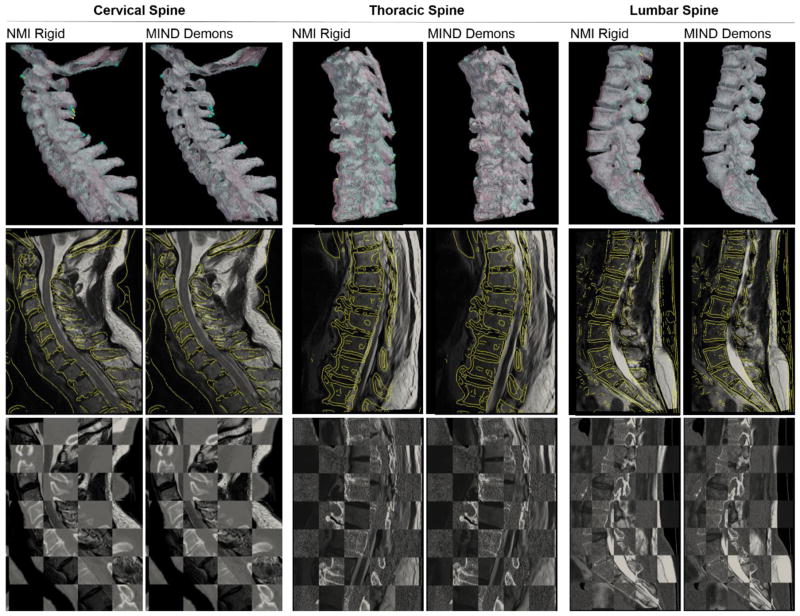
Result: The method yielded sub-voxel invertibility (0.006 mm) and nonsingular spatial Jacobians with capability to preserve local orientation and topology. It demonstrated improved registration accuracy in comparison to the reference methods, with mean target registration error (TRE) of 1.5 mm compared to 10.9, 2.3, and 4.6 mm for MI FFD, LMI FFD, and NMI Demons methods, respectively. Validation in clinical studies demonstrated realistic deformation with sub-voxel TRE in cases of cervical, thoracic, and lumbar spine.
Conclusions: A modality-independent deformable registration method has been developed to estimate a viscoelastic diffeomorphic map between preoperative MR and intraoperative CT. The method yields registration accuracy suitable to application in image-guided spine surgery across a broad range of anatomical sites and modes of deformation.
Keywords: CT; Demons algorithm; MIND; MRI; deformable image registration; image-guided surgery; multimodality image registration; symmetric diffeomorphism.
Figures
Similar articles
-
Performance evaluation of MIND demons deformable registration of MR and CT images in spinal interventions.Phys Med Biol. 2016 Dec 7;61(23):8276-8297. doi: 10.1088/0031-9155/61/23/8276. Epub 2016 Nov 3. Phys Med Biol. 2016. PMID: 27811396 Free PMC article.
-
MIND Demons: Symmetric Diffeomorphic Deformable Registration of MR and CT for Image-Guided Spine Surgery.IEEE Trans Med Imaging. 2016 Nov;35(11):2413-2424. doi: 10.1109/TMI.2016.2576360. Epub 2016 Jun 2. IEEE Trans Med Imaging. 2016. PMID: 27295656 Free PMC article.
-
A momentum-based diffeomorphic demons framework for deformable MR-CT image registration.Phys Med Biol. 2018 Oct 24;63(21):215006. doi: 10.1088/1361-6560/aae66c. Phys Med Biol. 2018. PMID: 30353886 Free PMC article.
-
Deformable image registration with local rigidity constraints for cone-beam CT-guided spine surgery.Phys Med Biol. 2014 Jul 21;59(14):3761-87. doi: 10.1088/0031-9155/59/14/3761. Epub 2014 Jun 17. Phys Med Biol. 2014. PMID: 24937093 Free PMC article.
-
Comparison of physics-based deformable registration methods for image-guided neurosurgery.Front Digit Health. 2023 Dec 8;5:1283726. doi: 10.3389/fdgth.2023.1283726. eCollection 2023. Front Digit Health. 2023. PMID: 38144260 Free PMC article. Review.
Cited by
-
SPIE Medical Imaging 50th anniversary: historical review of the Image-Guided Procedures, Robotic Interventions, and Modeling conference.J Med Imaging (Bellingham). 2022 Feb;9(Suppl 1):012206. doi: 10.1117/1.JMI.9.S1.012206. Epub 2022 Apr 18. J Med Imaging (Bellingham). 2022. PMID: 36225968 Free PMC article.
-
Inter-scanner Variation Independent Descriptors for Constrained Diffeomorphic Demons Registration of Retina OCT.Proc SPIE Int Soc Opt Eng. 2018 Feb;10574:105741B. doi: 10.1117/12.2293790. Epub 2018 Mar 2. Proc SPIE Int Soc Opt Eng. 2018. PMID: 31695241 Free PMC article.
-
Dose accumulation for MR-guided adaptive radiotherapy: From practical considerations to state-of-the-art clinical implementation.Front Oncol. 2023 Jan 26;12:1086258. doi: 10.3389/fonc.2022.1086258. eCollection 2022. Front Oncol. 2023. PMID: 36776378 Free PMC article. Review.
-
Performance evaluation of MIND demons deformable registration of MR and CT images in spinal interventions.Phys Med Biol. 2016 Dec 7;61(23):8276-8297. doi: 10.1088/0031-9155/61/23/8276. Epub 2016 Nov 3. Phys Med Biol. 2016. PMID: 27811396 Free PMC article.
-
Estimating tongue deformation during laryngoscopy using a hybrid FEM-multibody model and intraoperative tracking - a cadaver study.Comput Methods Biomech Biomed Engin. 2025 May;28(6):739-749. doi: 10.1080/10255842.2023.2301672. Epub 2024 Jan 9. Comput Methods Biomech Biomed Engin. 2025. PMID: 38193213
References
-
- Haldeman S, Kopansky-Giles D, Hurwitz EL, Hoy D, Mark Erwin W, Dagenais S, Kawchuk G, Strömqvist B, Walsh N. Advancements in the Management of Spine Disorders. Best Pract Res Clin Rheumatol. 2012;26(2):263–280. - PubMed
-
- Smith JS, Shaffrey CI, Glassman SD, Berven SH, Schwab FJ, Hamill CL, Horton WC, Ondra SL, Sansur CA, et al. Risk-benefit assessment of surgery for adult scoliosis: an analysis based on patient age. Spine (Phila Pa 1976) 2011;36(10):817–824. 2010/08/05 ed. - PubMed
-
- Larson AN, Polly DWJ, Guidera KJ, Mielke CH, Santos ERG, Ledonio CGT, Sembrano JN. The Accuracy of Navigation and 3D Image-Guided Placement for the Placement of Pedicle Screws in Congenital Spine Deformity. J Pediatr Orthop. 2012;32(6):e23–e29. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources