

Surgical management of skull base tumors
- PMID: 27330418
- PMCID: PMC4899518
- DOI: 10.1016/j.rpor.2014.09.002
Surgical management of skull base tumors
Abstract
Aim: To present a review of the contemporary surgical management of skull base tumors.
Background: Over the last two decades, the treatment of skull base tumors has evolved from observation, to partial resection combined with other therapy modalities, to gross total resection and no adjuvant treatment with good surgical results and excellent clinical outcomes.
Materials and methods: The literature review of current surgical strategies and management of skull base tumors was performed and complemented with the experience of Barrow Neurological Institute.
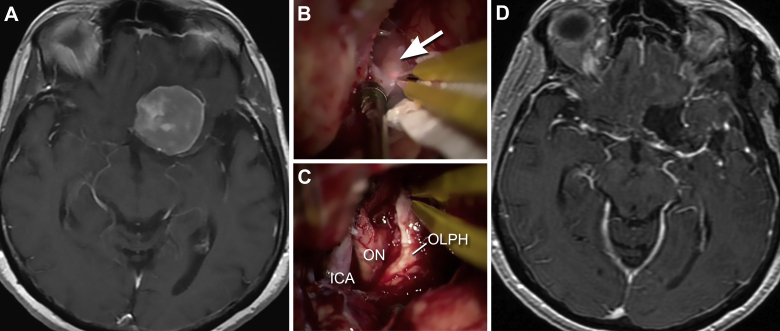
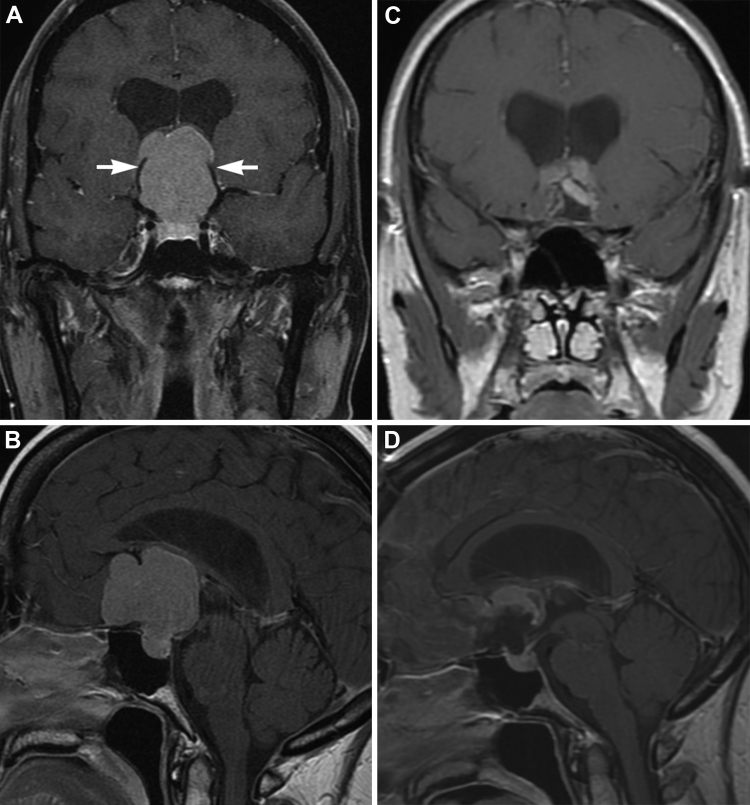
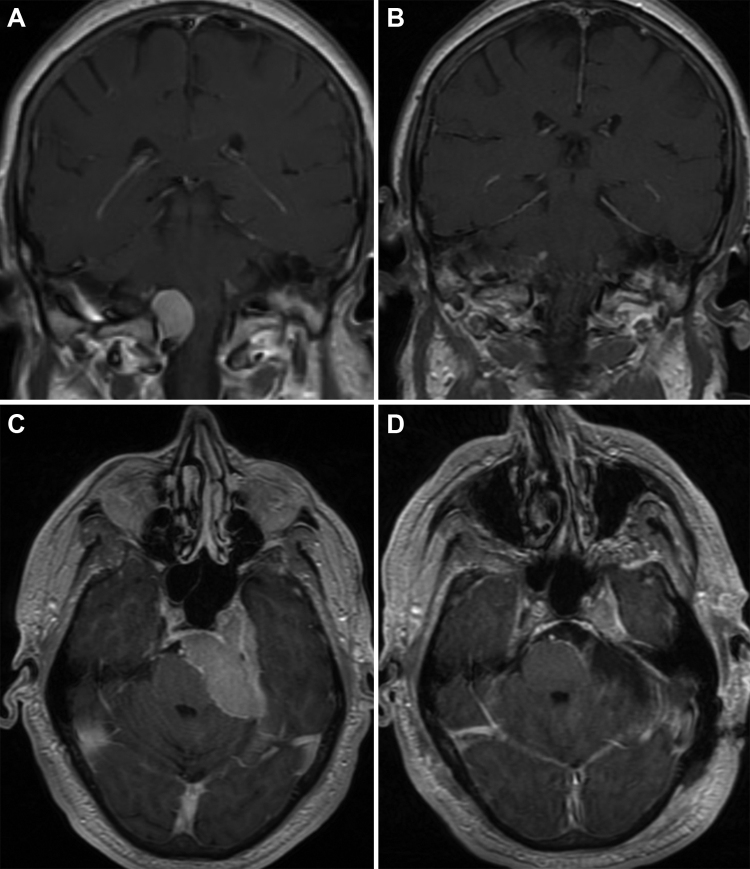
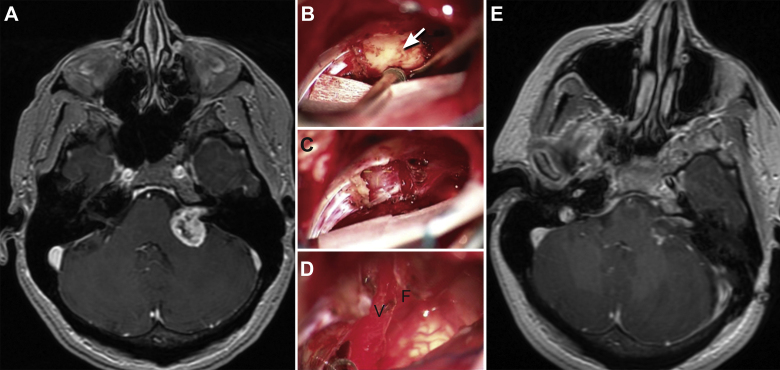
Results: Skull base tumors include meningiomas, pituitary tumors, sellar/parasellar tumors, vestibular and trigeminal schwannomas, esthesioneuroblastomas, chordomas, chondrosarcomas, and metastases. Surgical approaches include the modified orbitozygomatic, pterional, middle fossa, retrosigmoid, far lateral craniotomy, midline suboccipital craniotomy, and a combination of these approaches. The selection of an appropriate surgical approach depends on the characteristics of the patient and the tumor, as well as the experience of the neurosurgeon.
Conclusion: Modern microsurgical techniques, diagnostic imaging, intraoperative neuronavigation, and endoscopic technology have remarkably changed the concept of skull base surgery. These refinements have extended the boundaries of tumor resection with minimal morbidity.
Keywords: Meningoma; Neuroma; Schwannoma; Skull base; Skull base surgery.
Figures
References
-
- Spetzler R.F., Sanai N. The quiet revolution: retractorless surgery for complex vascular and skull base lesions. J Neurosurg. 2012;116(2):291–300. - PubMed
-
- Waring A.J., Housworth C.M., Voorhies R.M., Douglas J.R., Walker C.F., Connolly S.E. A prototype retractor system designed to minimize ischemic brain retractor injury: initial observations. Surg Neurol. 1990;34(3):139–143. - PubMed
-
- Yamaguchi M., Jadhav V., Obenaus A., Colohan A., Zhang J.H. Matrix metalloproteinase inhibition attenuates brain edema in an in vivo model of surgically induced brain injury. Neurosurgery. 2007;61(5):1067–1075. discussion 1075–6. - PubMed
-
- Ammirati M.Z.H. Oncology. In: Brem H., editor. vol. 2. Elsevier Saunders; Philadelphia: 2011. (Youmans neurological surgery).
LinkOut - more resources
Full Text Sources
Other Literature Sources
