

Undertriage of Trauma-Related Deaths in U.S. Emergency Departments
- PMID: 27330664
- PMCID: PMC4899063
- DOI: 10.5811/westjem.2016.2.29327
Undertriage of Trauma-Related Deaths in U.S. Emergency Departments
Abstract
Introduction: Accurate field triage of critically injured patients to trauma centers is vital for improving survival. We sought to estimate the national degree of undertriage of trauma patients who die in emergency departments (EDs) by evaluating the frequency and characteristics associated with triage to non-trauma centers.
Methods: This was a retrospective cross-sectional analysis of adult ED trauma deaths in the 2010 National Emergency Department Sample (NEDS). The primary outcome was appropriate triage to a trauma center (Level I, II or III) or undertriage to a non-trauma center. We subsequently focused on urban areas given improved access to trauma centers. We evaluated the associations of patient demographics, hospital region and mechanism of injury with triage to a trauma versus non-trauma center using multivariable logistic regression.
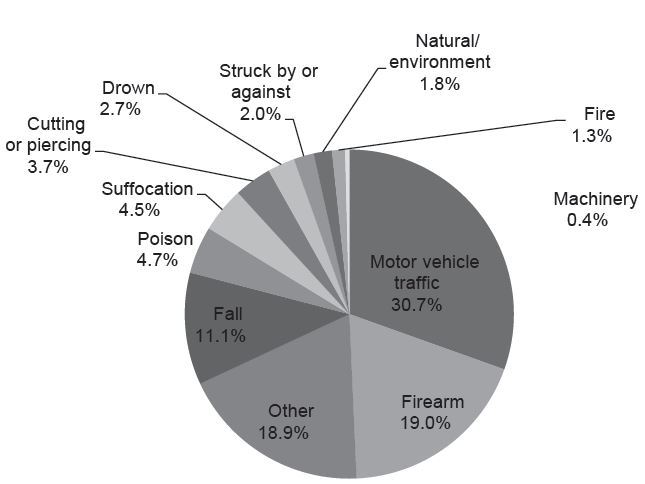
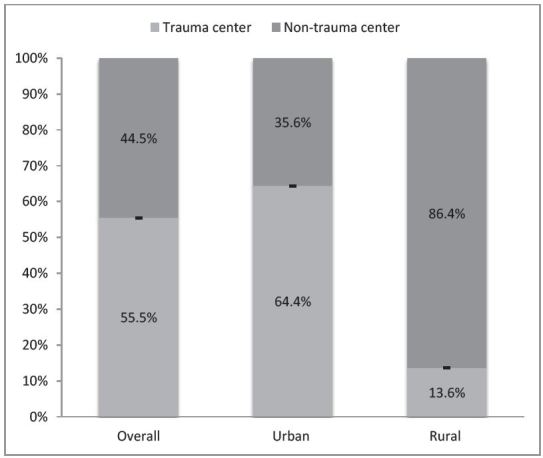
Results: We analyzed 3,971 included visits, representing 18,464 adult ED trauma-related deaths nationally. Of all trauma deaths, nearly half (44.5%, 95% CI [43.0-46.0]) of patients were triaged to non-trauma centers. In a subgroup analysis, over a third of urban ED visits (35.6%, 95% CI [34.1-37.1]) and most rural ED visits (86.4%, 95% CI [81.5-90.1]) were triaged to non-trauma centers. In urban EDs, female patients were less likely to be triaged to trauma centers versus non-trauma centers (adjusted odds ratio [OR] 0.83, 95% CI [0.70-0.99]). Highest median household income zip codes (≥$67,000) were less likely to be triaged to trauma centers than lowest median income ($1-40,999) (OR 0.54, 95% CI [0.43-0.69]). Compared to motor vehicle trauma, firearm trauma had similar odds of being triaged to a trauma center (OR 0.90, 95% CI [0.71-1.14]); however, falls were less likely to be triaged to a trauma center (OR 0.50, 95 %CI [0.38-0.66]).
Conclusion: We found that nearly half of all trauma patients nationally and one-third of urban trauma patients, who died in the ED, were triaged to non-trauma centers, and thus undertriaged. Sex and other demographic disparities associated with this triage decision represent targeted opportunities to improve our trauma systems and reduce undertriage.
Figures
References
-
- Eastman AB, Lewis FR, Jr, Champion HR, et al. Regional trauma system design: critical concepts. Am J Surg. 1987;154:79–87. - PubMed
-
- MacKenzie EJ, Rivara FP, Jurkovich GJ, et al. A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006;354:366–78. - PubMed
-
- Celso B, Tepas J, Langland-Orban B, et al. A systematic review and meta-analysis comparing outcome of severely injured patients treated in trauma centers following the establishment of trauma systems. J Trauma. 2006;60:371–8. - PubMed
-
- Nathens AB, Jurkovich GJ, Rivara FP, et al. Effectiveness of state trauma systems in reducing injury-related mortality: a national evaluation. J Trauma. 2000;48:25–30. - PubMed
-
- Kane G, Engelhardt R, Celentano J, et al. Empirical development and evaluation of prehospital trauma triage instruments. J Trauma. 1985;25:482–9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
