

The Molecular and Spatial Epidemiology of Typhoid Fever in Rural Cambodia
- PMID: 27331909
- PMCID: PMC4917249
- DOI: 10.1371/journal.pntd.0004785
The Molecular and Spatial Epidemiology of Typhoid Fever in Rural Cambodia
Abstract
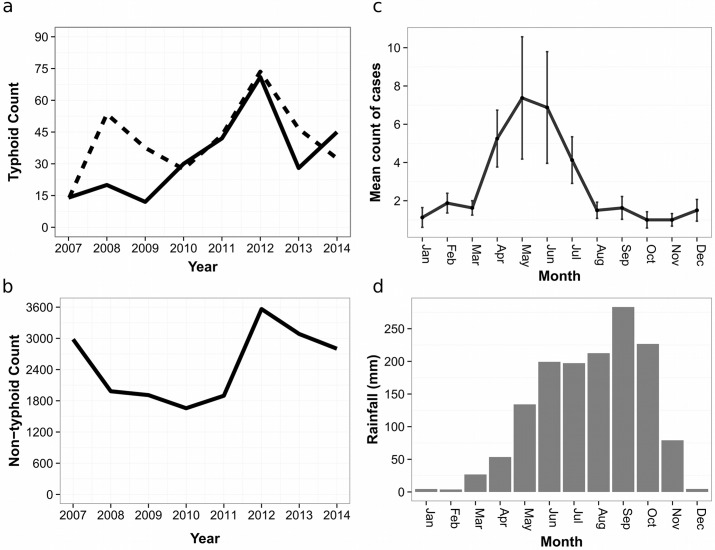
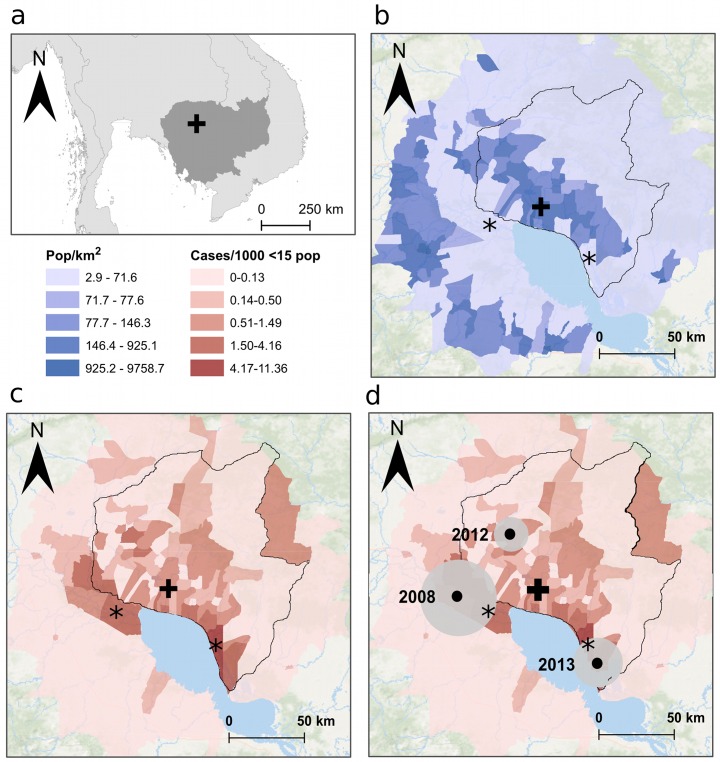
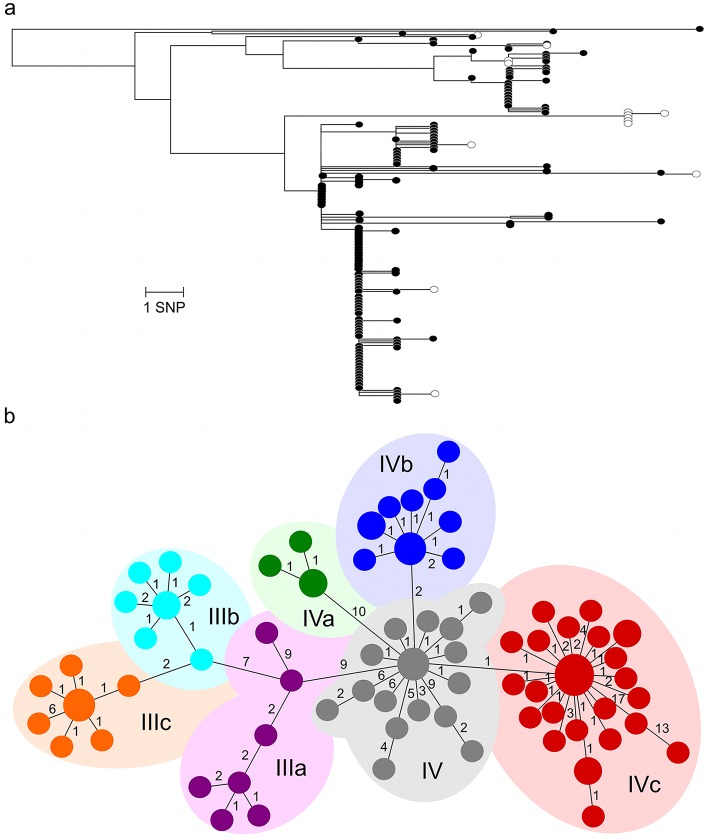
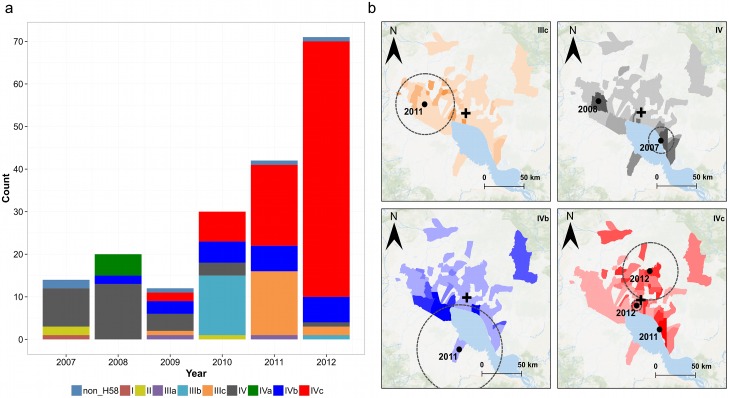
Typhoid fever, caused by the bacterium Salmonella Typhi, is an endemic cause of febrile disease in Cambodia. The aim of this study was to better understand the epidemiology of pediatric typhoid fever in Cambodia. We accessed routine blood culture data from Angkor Hospital for Children (AHC) in Siem Reap province between 2007 and 2014, and performed whole genome sequencing (WGS) on the isolated bacteria to characterize the S. Typhi population. The resulting phylogenetic information was combined with conventional epidemiological approaches to investigate the spatiotemporal distribution of S. Typhi and population-level risk factors for reported disease. During the study period, there were 262 cases of typhoid within a 100 km radius of AHC, with a median patient age of 8.2 years (IQR: 5.1-11.5 years). The majority of infections occurred during the rainy season, and commune incidences as high as 11.36/1,000 in children aged <15 years were observed over the study period. A population-based risk factor analysis found that access to water within households and increasing distance from Tonle Sap Lake were protective. Spatial mapping and WGS provided additional resolution for these findings, and confirmed that proximity to the lake was associated with discrete spatiotemporal disease clusters. We confirmed the dominance of MDR H58 S. Typhi in this population, and found substantial evidence of diversification (at least seven sublineages) within this single lineage. We conclude that there is a substantial burden of pediatric typhoid fever in rural communes in Cambodia. Our data provide a platform for additional population-based typhoid fever studies in this location, and suggest that this would be a suitable setting in which to introduce a school-based vaccination programme with Vi conjugate vaccines.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Schwartz E (2010) Typhoid and Paratyphoid Fever. Trop Dis Travel 366: 144–153.
-
- World Health Organization (2003) Background document: The diagnosis, treatment and prevention of typhoid fever. World Health Organization: 38.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
