

Review
doi: 10.1259/bjr.20160221.
Epub 2016 Jun 22.
Abdominal manifestations of histiocytic disorders in adults: imaging perspective
Affiliations
- PMID: 27332519
- PMCID: PMC5124924
- DOI: 10.1259/bjr.20160221
Item in Clipboard
Review
Abdominal manifestations of histiocytic disorders in adults: imaging perspective
Br J Radiol.
2016 Sep.
Abstract
Histiocytic disorders (HDs) are a diverse group of diseases characterized by pathologic infiltration of normal tissues by cells of the mononuclear phagocyte system. The spectrum of these diseases ranges from treatable infectious diseases to rapidly progressive, life-threatening conditions. Although they are rare and difficult diagnoses, HDs can be diagnosed with the help of clinical and laboratory analyses, imaging features and tissue biopsy. The clinicopathology and imaging spectrum of select entities belonging to this disorder are presented in this review.
Figures

A 34-year-old male with history of cigarette smoking presenting with cough and diarrhoea: (a) the coronal CT image of the chest is demonstrating multiple cavities with varying and bizarre shapes with upper lobe predominance (arrow). (b) Contrast-enhanced CT of the abdomen is demonstrating periportal hypodense areas (arrow). Ultrasound-guided biopsy of this periportal lesion confirmed diagnosis of Langerhans cell histiocytosis.
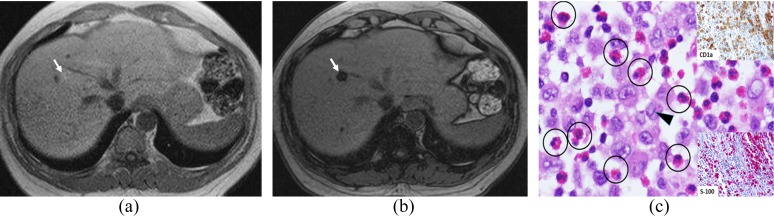
A 39-year-old male with biopsy-proven Langerhans cell histiocytosis of the liver: (a) subtle hyperintense lesions can be seen on the GRE T1 weighted (T1W) in-phase MR image (arrow) with signal drop on the GRE T1W opposed-phase MR image (arrow) (b) consistent with intracytoplasmic fat in these lesions. (c) Biopsy of the liver lesions showing diffuse infiltrates of loosely dispersed Langerhans cells (LC) with convoluted or grooved nuclei (arrowhead), fine chromatin pattern and eosinophilic cytoplasm. Admixed with the LC are many eosinophils (circles). The LC are positive for CD1a (right upper insert) and S-100 (right lower insert).
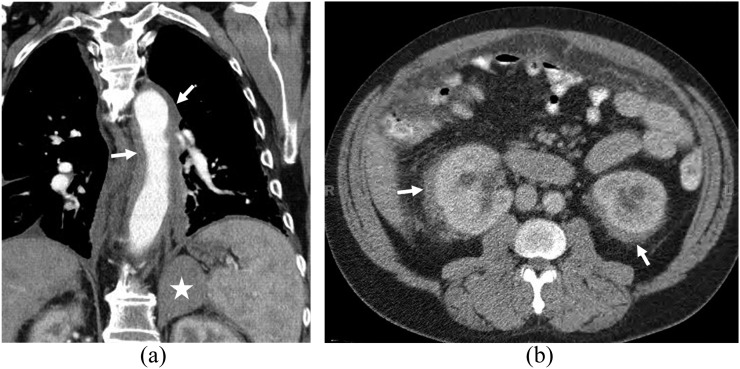
A 45-year-old male with Erdheim–Chester disease: (a) the contrast-enhanced coronal and (b) axial images are demonstrating a diffuse soft-tissue rind surrounding the thoracic and abdominal aorta, giving rise to a “coated aorta” appearance [arrows in (a)]. Left adrenal mass can also be seen (star). (b) Bilateral perinephric soft-tissue infiltration is seen with “hairy kidney” appearance (arrows).
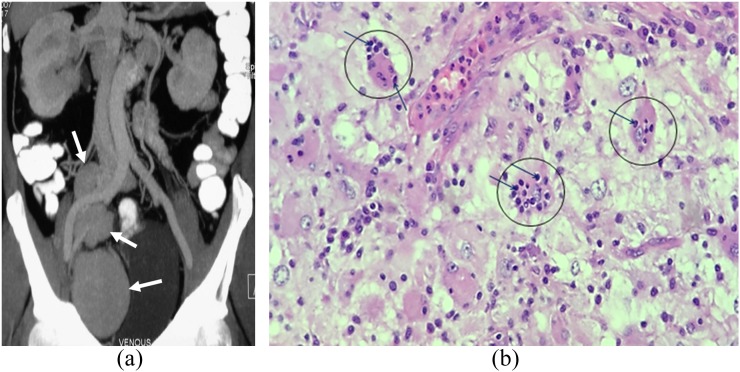
A 22-year-old male with Rosai–Dorfman disease: (a) the contrast-enhanced axial coronal maximum intensity projection CT image is demonstrating multiple enhancing masses in the right pelvis (arrows). (b) Histologic section from the resected pelvic lymph node is showing large histiocytes (circles) with the characteristic “emperipolesis”, in which intact lymphocytes (arrows) are present in the cytoplasm of the histiocytes.
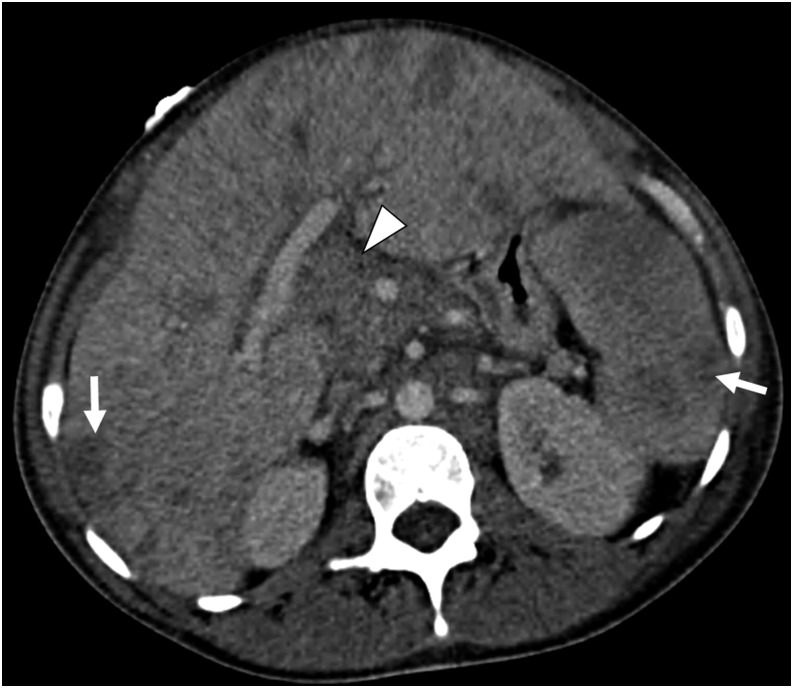
A 30-year-old female with haemophagocytic lymphohistiocytosis presenting with septic shock: the axial contrast-enhanced CT image is demonstrating hepatosplenomegaly and innumerable hypodense hepatic and splenic lesions (arrows). Periportal lymphadenopathy is also seen (arrowhead). Histopathology confirmed the diagnosis on transjugular liver biopsy.

A 52-year-old male with xanthogranulomatous inflammation of the transverse colon, mesocolon and omentum: (a) the axial contrast-enhanced CT image is demonstrating a large, heterogeneous, infiltrating mass in the omentum (arrow), also involving the transverse colon (asterisk) and its mesocolon. (b) Histopathology after surgical resection revealing xanthogranulomatous infiltrates in the omentum (area inside the square) with foamy histiocytes infiltrating into the adjacent bowel and mesentery.
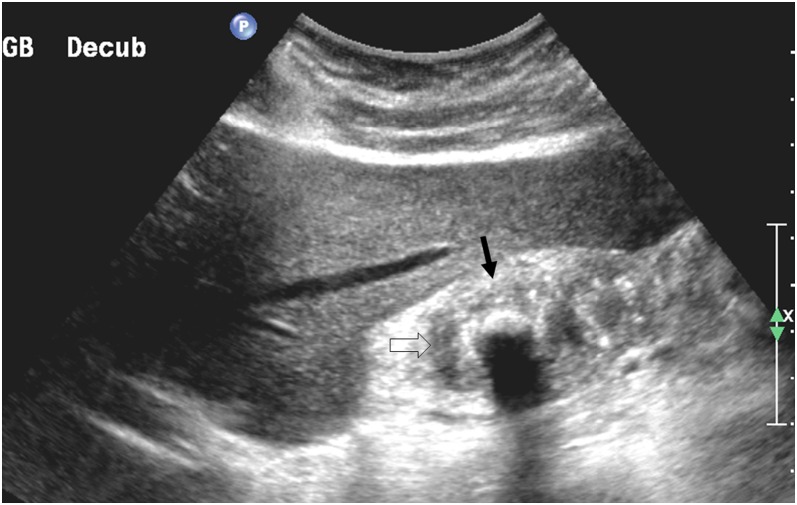
A 46-year-old female with xanthogranulomatous cholecystitis: the right upper quadrant sonogram is showing marked thickening of the gall bladder wall (arrow) with hypoechoic areas within the thickened wall (open arrow) associated with gallstones.
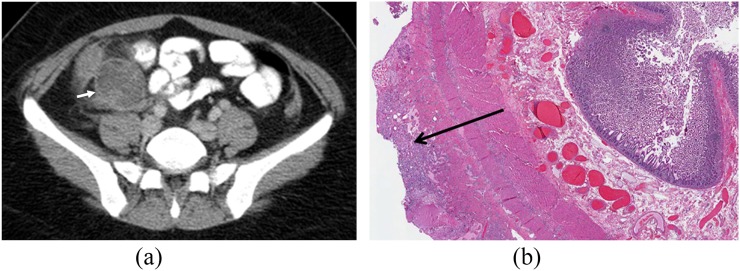
A 24-year-old male with xanthogranulomatous appendicitis: (a) the axial contrast-enhanced CT image is demonstrating pericaecal fluid collection (arrow) not seen separate from the appendix. (b) The histopathology slide at low magnification demonstrating serosal xanthogranulomatous inflammation (arrow) in the serosa of the resected bowel wall.
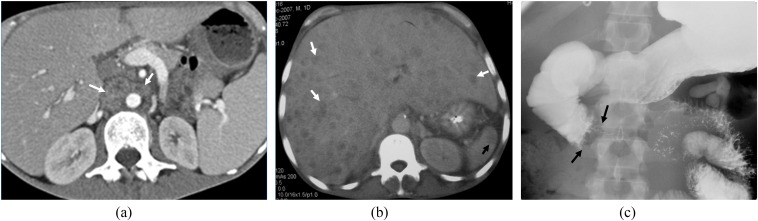
Imaging spectrum of mycobacterium avium complex infection in three different patients: (a) contrast-enhanced axial CT image demonstrating small periaortic necrotic lymph nodes (white arrows); (b) multiple hypodense hepatic lesions (white arrows) and splenic lesions (black arrows) are seen in contrast-enhanced axial CT; and (c) diffuse mass-like wall thickening involving the duodenum causing partial obstruction (black arrows) is seen on the small bowel follow-through barium examination.

A 52-year-old male with Whipple disease: the image from a small bowel follow-through fluoroscopic barium examination is showing diffuse nodular, thickened and irregular folds, predominantly involving the jejunum and, to a lesser degree, the ileum.

An 82-year-old female with abdominal pain and barium granuloma: a fat density mass-like lesion is seen in the pelvis on the coronal CT image (arrowheads). High-density extraluminal barium is seen in the peritoneal cavity from prior perforation during a barium enema. Histopathology at resection showing a multinucleated giant cell with engulfed polarizing crystals.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
