

Intraoperative Supine Breast MR Imaging to Quantify Tumor Deformation and Detection of Residual Breast Cancer: Preliminary Results
- PMID: 27332738
- PMCID: PMC5118055
- DOI: 10.1148/radiol.2016151472
Intraoperative Supine Breast MR Imaging to Quantify Tumor Deformation and Detection of Residual Breast Cancer: Preliminary Results
Abstract
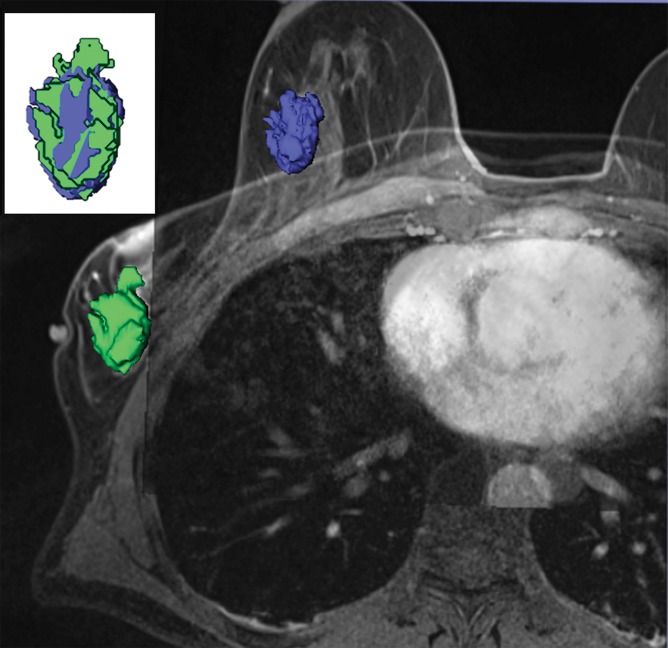
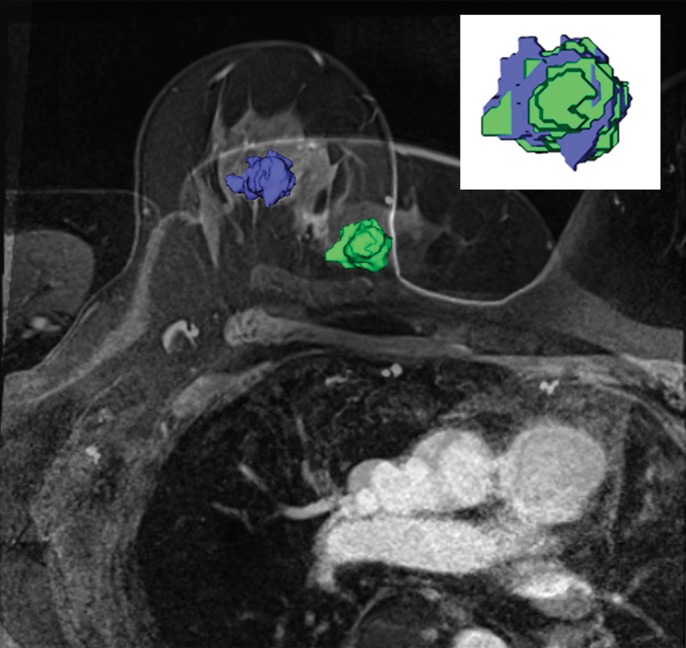
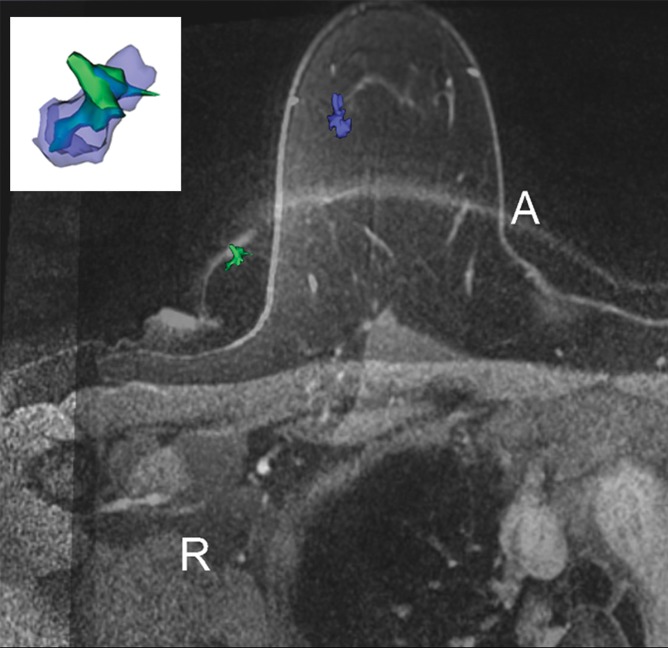
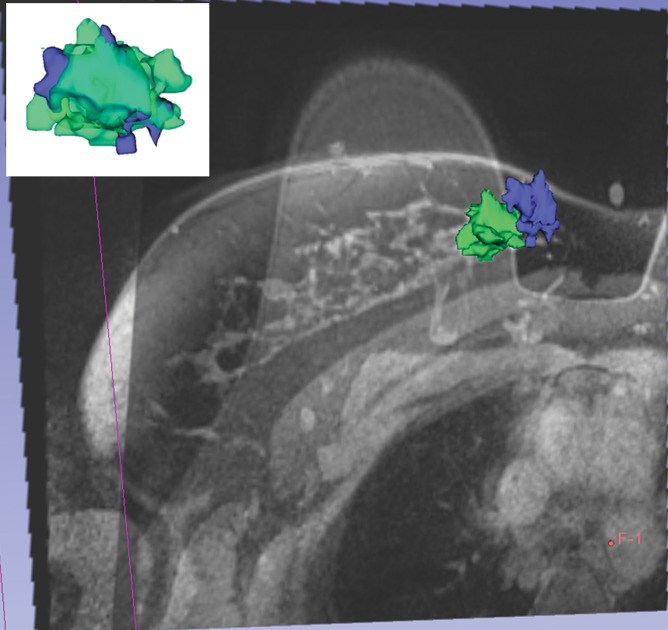
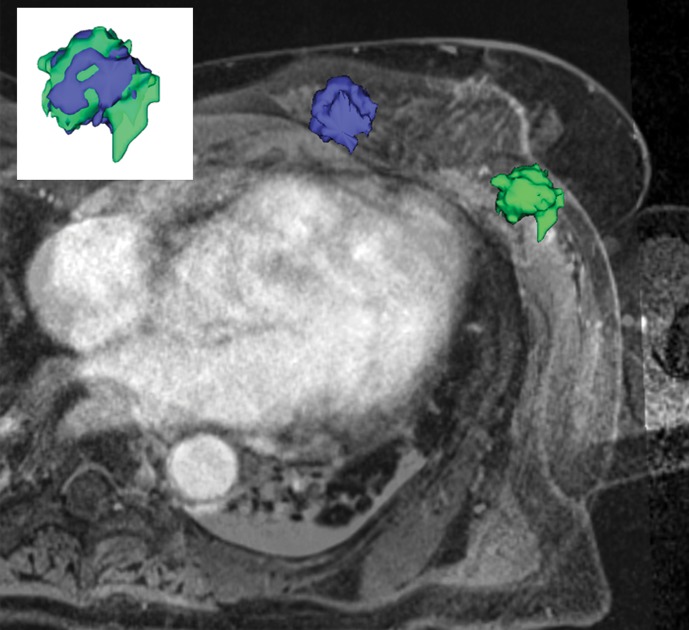
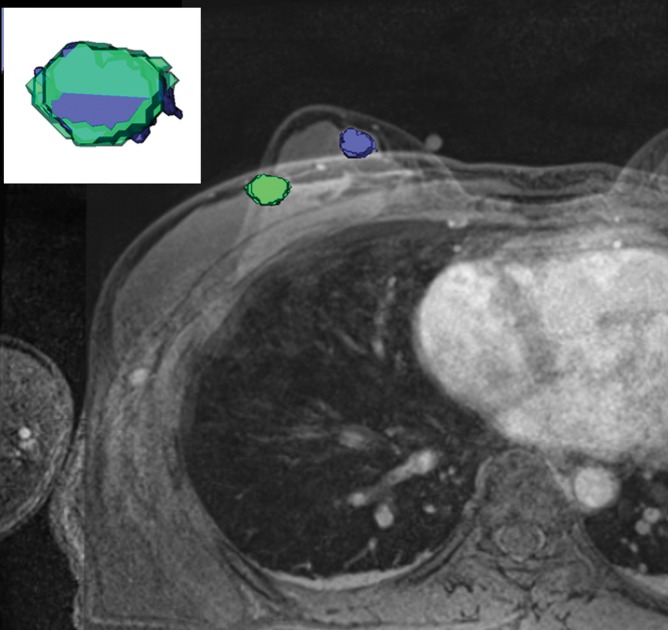
Purpose To use intraoperative supine magnetic resonance (MR) imaging to quantify breast tumor deformation and displacement secondary to the change in patient positioning from imaging (prone) to surgery (supine) and to evaluate residual tumor immediately after breast-conserving surgery (BCS). Materials and Methods Fifteen women gave informed written consent to participate in this prospective HIPAA-compliant, institutional review board-approved study between April 2012 and November 2014. Twelve patients underwent lumpectomy and postsurgical intraoperative supine MR imaging. Six of 12 patients underwent both pre- and postsurgical supine MR imaging. Geometric, structural, and heterogeneity metrics of the cancer and distances of the tumor from the nipple, chest wall, and skin were computed. Mean and standard deviations of the changes in volume, surface area, compactness, spherical disproportion, sphericity, and distances from key landmarks were computed from tumor models. Imaging duration was recorded. Results The mean differences in tumor deformation metrics between prone and supine imaging were as follows: volume, 23.8% (range, -30% to 103.95%); surface area, 6.5% (range, -13.24% to 63%); compactness, 16.2% (range, -23% to 47.3%); sphericity, 6.8% (range, -9.10% to 20.78%); and decrease in spherical disproportion, -11.3% (range, -60.81% to 76.95%). All tumors were closer to the chest wall on supine images than on prone images. No evidence of residual tumor was seen on MR images obtained after the procedures. Mean duration of pre- and postoperative supine MR imaging was 25 minutes (range, 18.4-31.6 minutes) and 19 minutes (range, 15.1-22.9 minutes), respectively. Conclusion Intraoperative supine breast MR imaging, when performed in conjunction with standard prone breast MR imaging, enables quantification of breast tumor deformation and displacement secondary to changes in patient positioning from standard imaging (prone) to surgery (supine) and may help clinicians evaluate for residual tumor immediately after BCS. © RSNA, 2016 Online supplemental material is available for this article.
Conflict of interest statement
are listed at the end of this article. Disclosures of Conflicts of Interest: E.C.G. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: received royalties from Amirsys Publishing. Other relationships: disclosed no relevant relationships. J.J. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: received grants from Siemens and Symbow Medical; has multiple patents pending. Other relationships: disclosed no relevant relationships. D.M.R. disclosed no relevant relationships. D.L.C. disclosed no relevant relationships. M.A.M. disclosed no relevant relationships. F.A.J. disclosed no relevant relationships. M.G. disclosed no relevant relationships.
Figures
References
-
- Camp ER, McAuliffe PF, Gilroy JS, et al. Minimizing local recurrence after breast conserving therapy using intraoperative shaved margins to determine pathologic tumor clearance. J Am Coll Surg 2005;201(6):855–861. - PubMed
-
- Cowen D, Houvenaeghel G, Bardou V, et al. Local and distant failures after limited surgery with positive margins and radiotherapy for node-negative breast cancer. Int J Radiat Oncol Biol Phys 2000;47(2):305–312. - PubMed
-
- Menes TS, Tartter PI, Bleiweiss I, Godbold JH, Estabrook A, Smith SR. The consequence of multiple re-excisions to obtain clear lumpectomy margins in breast cancer patients. Ann Surg Oncol 2005;12(11):881–885. - PubMed
-
- Russo AL, Arvold ND, Niemierko A, et al. Margin status and the risk of local recurrence in patients with early-stage breast cancer treated with breast-conserving therapy. Breast Cancer Res Treat 2013;140(2):353–361. - PubMed
-
- Sabel MS, Rogers K, Griffith K, et al. Residual disease after re-excision lumpectomy for close margins. J Surg Oncol 2009;99(2):99–103. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
