

Effect of exercise training on ventilatory efficiency in patients with heart disease: a review
- PMID: 27332771
- PMCID: PMC4918788
- DOI: 10.1590/1414-431X20165180
Effect of exercise training on ventilatory efficiency in patients with heart disease: a review
Abstract
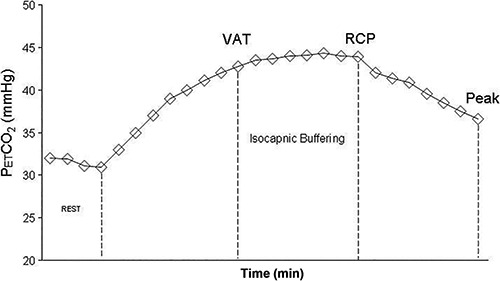
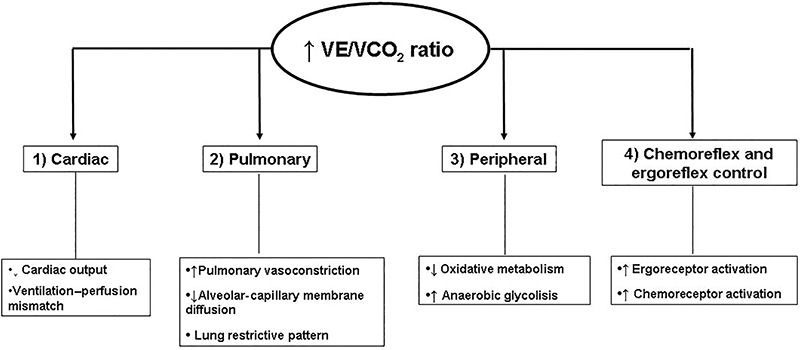
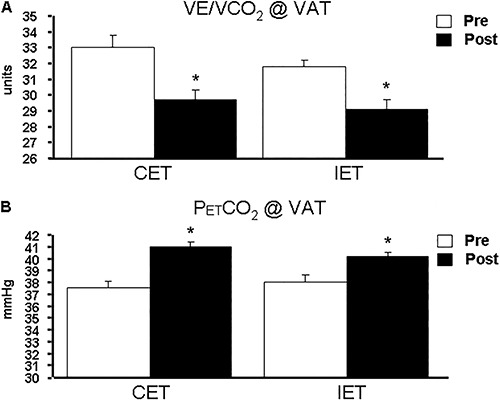
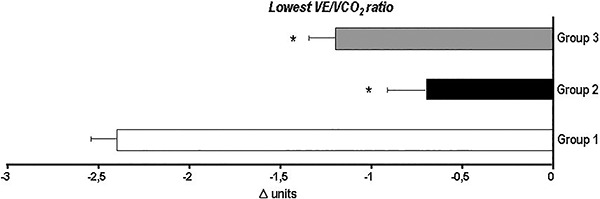
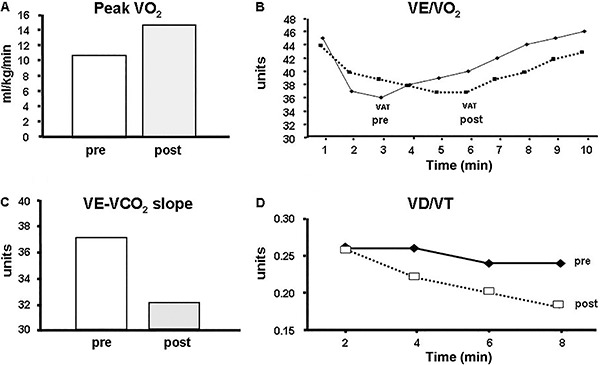
The analysis of ventilatory efficiency in cardiopulmonary exercise testing has proven useful for assessing the presence and severity of cardiorespiratory diseases. During exercise, efficient pulmonary gas exchange is characterized by uniform matching of lung ventilation with perfusion. By contrast, mismatching is marked by inefficient pulmonary gas exchange, requiring increased ventilation for a given CO2 production. The etiology of increased and inefficient ventilatory response to exercise in heart disease is multifactorial, involving both peripheral and central mechanisms. Exercise training has been recommended as non-pharmacological treatment for patients with different chronic cardiopulmonary diseases. In this respect, previous studies have reported improvements in ventilatory efficiency after aerobic exercise training in patients with heart disease. Against this background, the primary objective of the present review was to discuss the pathophysiological mechanisms involved in abnormal ventilatory response to exercise, with an emphasis on both patients with heart failure syndrome and coronary artery disease. Secondly, special focus was dedicated to the role of aerobic exercise training in improving indices of ventilatory efficiency among these patients, as well as to the underlying mechanisms involved.
Figures

References
-
- Wasserman K. Cardiopulmonary exercise testing and cardiovascular health. Armonk: Futura; 2002.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
