

Development of Upper Respiratory Tract Microbiota in Infancy is Affected by Mode of Delivery
- PMID: 27333043
- PMCID: PMC4972531
- DOI: 10.1016/j.ebiom.2016.05.031
Development of Upper Respiratory Tract Microbiota in Infancy is Affected by Mode of Delivery
Abstract
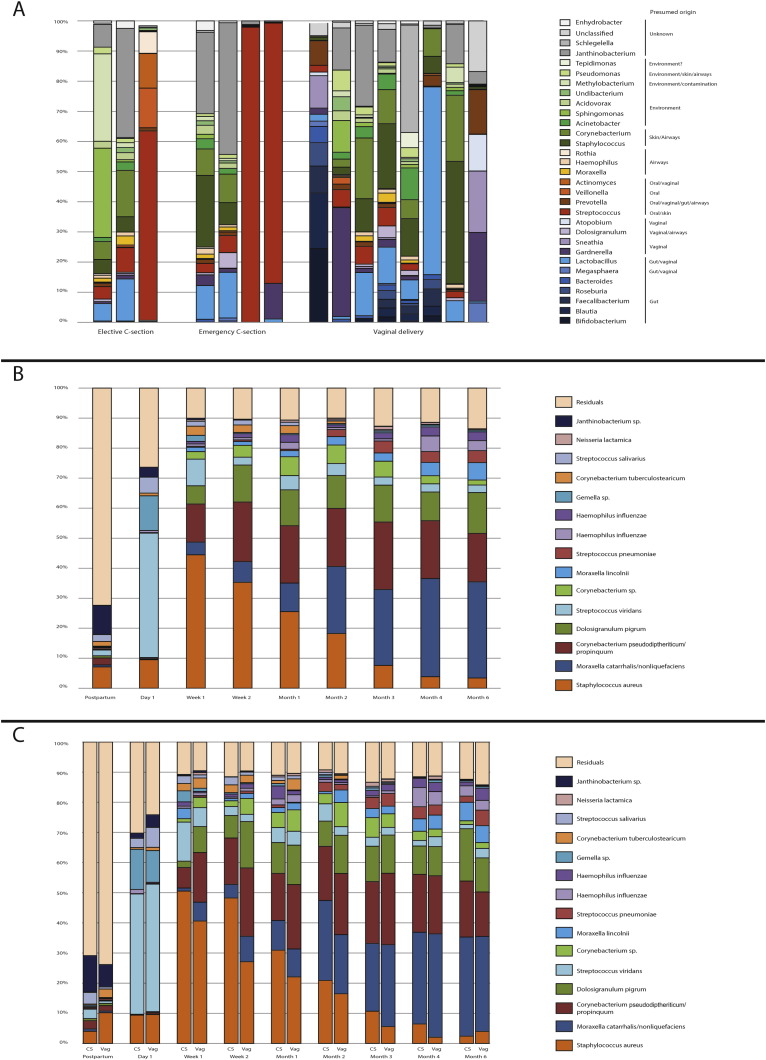
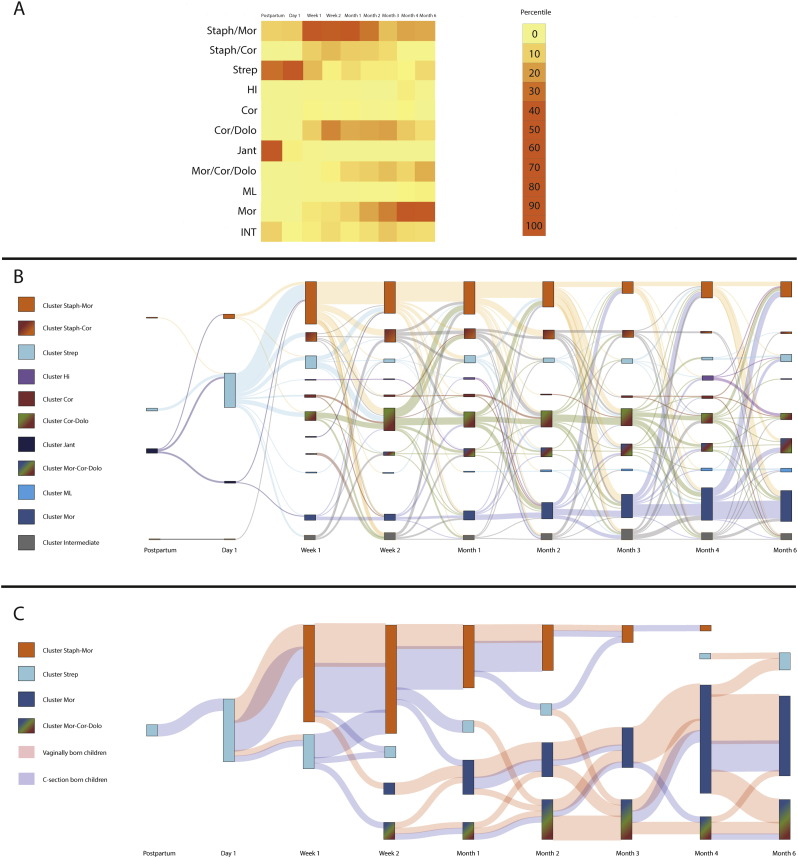
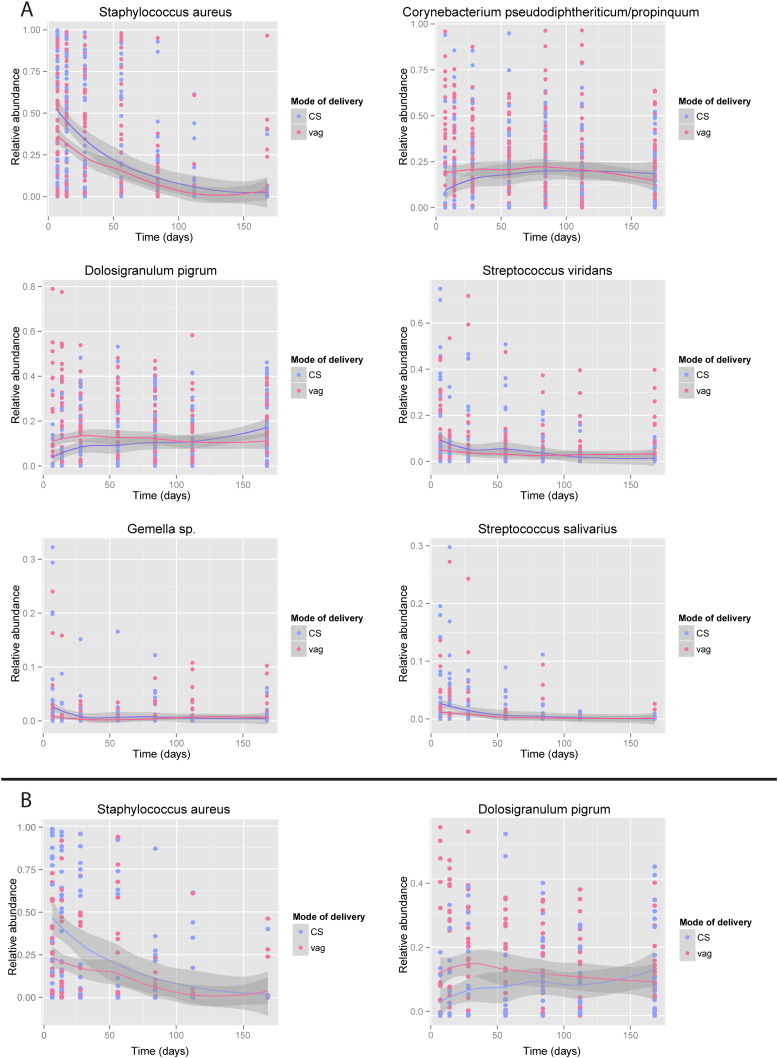
Birth by Caesarian section is associated with short- and long-term respiratory morbidity. We hypothesized that mode of delivery affects the development of the respiratory microbiota, thereby altering its capacity to provide colonization resistance and consecutive pathobiont overgrowth and infections. Therefore, we longitudinally studied the impact of mode of delivery on the nasopharyngeal microbiota development from birth until six months of age in a healthy, unselected birth cohort of 102 children (n=761 samples). Here, we show that the respiratory microbiota develops within one day from a variable mixed bacterial community towards a Streptococcus viridans-predominated profile, regardless of mode of delivery. Within the first week, rapid niche differentiation had occurred; initially with in most infants Staphylococcus aureus predominance, followed by differentiation towards Corynebacterium pseudodiphteriticum/propinquum, Dolosigranulum pigrum, Moraxella catarrhalis/nonliquefaciens, Streptococcus pneumoniae, and/or Haemophilus influenzae dominated communities. Infants born by Caesarian section showed a delay in overall development of respiratory microbiota profiles with specifically reduced colonization with health-associated commensals like Corynebacterium and Dolosigranulum, thereby possibly influencing respiratory health later in life.
Keywords: Caesarian section; Microbiome; Microbiota; Mode of delivery; Respiratory tract; Respiratory tract infection.
Copyright © 2016 The Authors. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Biesbroek G., Bosch A.A.T.M., Wang X., Keijser B.J.F., Veenhoven R.H., Sanders E.A.M., Bogaert D. The impact of breastfeeding on nasopharyngeal microbial communities in infants. Am. J. Respir. Crit. Care Med. 2014;190:298–308. - PubMed
-
- Biesbroek G., Tsivtsivadze E., Sanders E.A.M., Montijn R., Veenhoven R.H., Keijser B.J.F., Bogaert D. Early respiratory microbiota composition determines bacterial succession patterns and respiratory health in children. Am. J. Respir. Crit. Care Med. 2014 - PubMed
-
- Bosch A.A.T.M., van Houten M.A., Bruin J.P., Wijmenga-Monsuur A.J., Trzciński K., Bogaert D., Rots N.Y., Sanders E.A.M. Nasopharyngeal carriage of Streptococcus pneumoniae and other bacteria in the 7th year after implementation of the pneumococcal conjugate vaccine in the Netherlands. Vaccine. 2015;34:531–539. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
