

Evaluation of 12 strategies for obtaining second opinions to improve interpretation of breast histopathology: simulation study
- PMID: 27334105
- PMCID: PMC4916777
- DOI: 10.1136/bmj.i3069
Evaluation of 12 strategies for obtaining second opinions to improve interpretation of breast histopathology: simulation study
Abstract
Objective: To evaluate the potential effect of second opinions on improving the accuracy of diagnostic interpretation of breast histopathology.
Design: Simulation study.
Setting: 12 different strategies for acquiring independent second opinions.
Participants: Interpretations of 240 breast biopsy specimens by 115 pathologists, one slide for each case, compared with reference diagnoses derived by expert consensus.
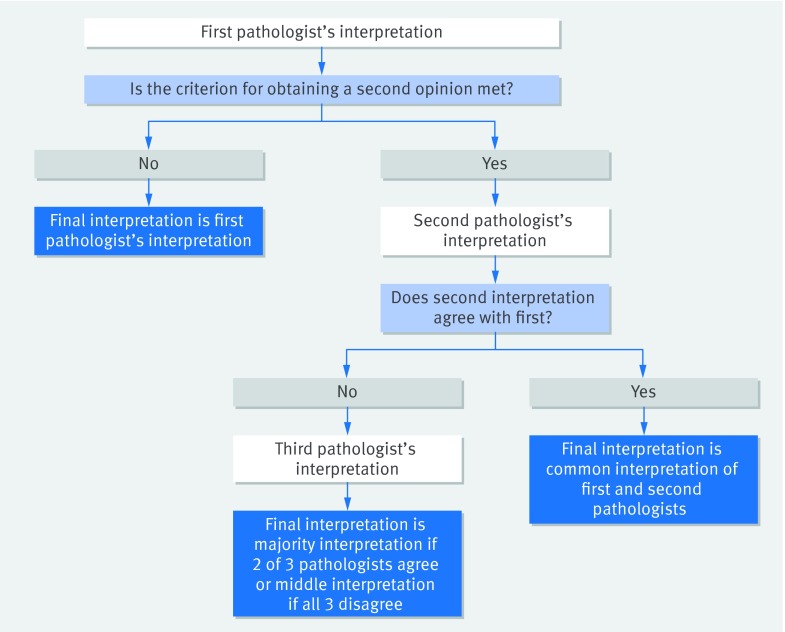
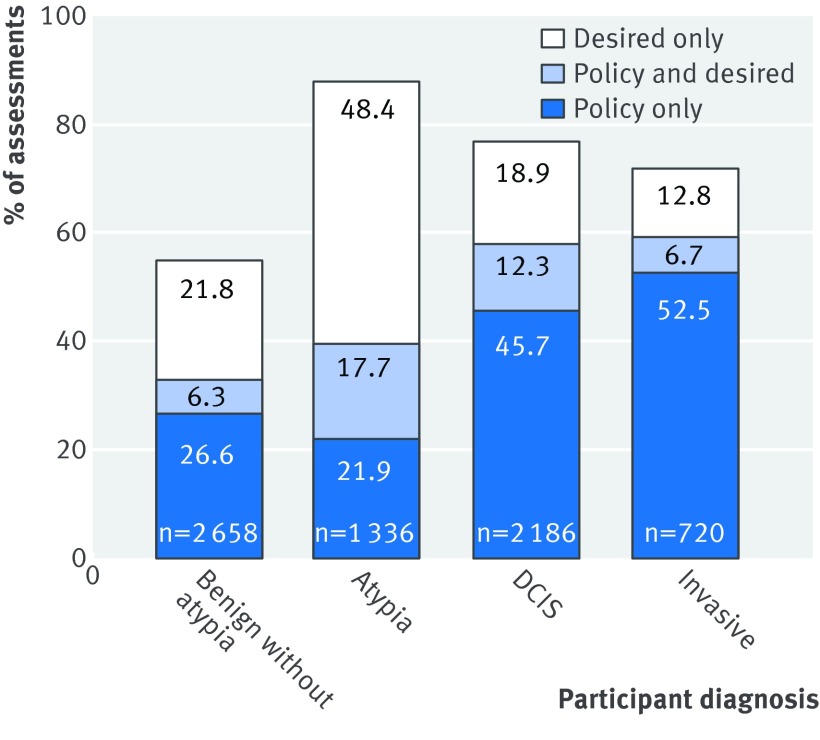
Main outcome measures: Misclassification rates for individual pathologists and for 12 simulated strategies for second opinions. Simulations compared accuracy of diagnoses from single pathologists with that of diagnoses based on pairing interpretations from first and second independent pathologists, where resolution of disagreements was by an independent third pathologist. 12 strategies were evaluated in which acquisition of second opinions depended on initial diagnoses, assessment of case difficulty or borderline characteristics, pathologists' clinical volumes, or whether a second opinion was required by policy or desired by the pathologists. The 240 cases included benign without atypia (10% non-proliferative, 20% proliferative without atypia), atypia (30%), ductal carcinoma in situ (DCIS, 30%), and invasive cancer (10%). Overall misclassification rates and agreement statistics depended on the composition of the test set, which included a higher prevalence of difficult cases than in typical practice.
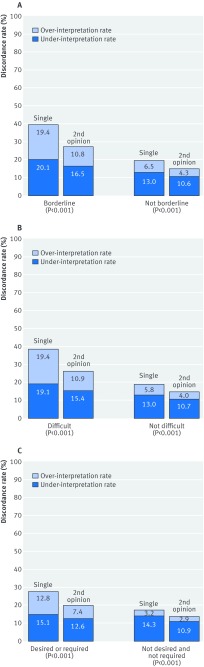
Results: Misclassification rates significantly decreased (P<0.001) with all second opinion strategies except for the strategy limiting second opinions only to cases of invasive cancer. The overall misclassification rate decreased from 24.7% to 18.1% when all cases received second opinions (P<0.001). Obtaining both first and second opinions from pathologists with a high volume (≥10 breast biopsy specimens weekly) resulted in the lowest misclassification rate in this test set (14.3%, 95% confidence interval 10.9% to 18.0%). Obtaining second opinions only for cases with initial interpretations of atypia, DCIS, or invasive cancer decreased the over-interpretation of benign cases without atypia from 12.9% to 6.0%. Atypia cases had the highest misclassification rate after single interpretation (52.2%), remaining at more than 34% in all second opinion scenarios.
Conclusion: Second opinions can statistically significantly improve diagnostic agreement for pathologists' interpretations of breast biopsy specimens; however, variability in diagnosis will not be completely eliminated, especially for breast specimens with atypia.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
"Take two"? The role of second opinions for breast biopsy specimens.BMJ. 2016 Jun 23;353:i3256. doi: 10.1136/bmj.i3256. BMJ. 2016. PMID: 27339037 No abstract available.
-
Digital pathology imaging offers more benefits than glass slides and microscopes.BMJ. 2016 Jul 12;354:i3813. doi: 10.1136/bmj.i3813. BMJ. 2016. PMID: 27406811 No abstract available.
Similar articles
-
Diagnostic concordance among pathologists interpreting breast biopsy specimens.JAMA. 2015 Mar 17;313(11):1122-32. doi: 10.1001/jama.2015.1405. JAMA. 2015. PMID: 25781441 Free PMC article.
-
The diagnostic challenge of low-grade ductal carcinoma in situ.Eur J Cancer. 2017 Jul;80:39-47. doi: 10.1016/j.ejca.2017.04.013. Epub 2017 May 20. Eur J Cancer. 2017. PMID: 28535496 Free PMC article.
-
Variability in Pathologists' Interpretations of Individual Breast Biopsy Slides: A Population Perspective.Ann Intern Med. 2016 May 17;164(10):649-55. doi: 10.7326/M15-0964. Epub 2016 Mar 22. Ann Intern Med. 2016. PMID: 26999810 Free PMC article.
-
Atypia in breast pathology: what pathologists need to know.Pathology. 2022 Feb;54(1):20-31. doi: 10.1016/j.pathol.2021.09.008. Epub 2021 Dec 3. Pathology. 2022. PMID: 34872753 Review.
-
Borderline breast lesions: diagnostic challenges and clinical implications.Adv Anat Pathol. 2011 May;18(3):190-8. doi: 10.1097/PAP.0b013e31821698cc. Adv Anat Pathol. 2011. PMID: 21490436 Review.
Cited by
-
Assessment of Second-Opinion Strategies for Diagnoses of Cutaneous Melanocytic Lesions.JAMA Netw Open. 2019 Oct 2;2(10):e1912597. doi: 10.1001/jamanetworkopen.2019.12597. JAMA Netw Open. 2019. PMID: 31603483 Free PMC article.
-
Variability in grading of ductal carcinoma in situ among an international group of pathologists.J Pathol Clin Res. 2021 May;7(3):233-242. doi: 10.1002/cjp2.201. Epub 2021 Feb 23. J Pathol Clin Res. 2021. PMID: 33620141 Free PMC article.
-
Characteristics associated with requests by pathologists for second opinions on breast biopsies.J Clin Pathol. 2017 Nov;70(11):947-953. doi: 10.1136/jclinpath-2016-204231. Epub 2017 May 2. J Clin Pathol. 2017. PMID: 28465449 Free PMC article.
-
Helicobacter pylori Eradication for Metachronous Gastric Cancer: An Unsuitable Methodology Impeding Broader Clinical Usage.Front Oncol. 2019 Feb 20;9:90. doi: 10.3389/fonc.2019.00090. eCollection 2019. Front Oncol. 2019. PMID: 30842937 Free PMC article. No abstract available.
-
Second opinion strategies in breast pathology: a decision analysis addressing over-treatment, under-treatment, and care costs.Breast Cancer Res Treat. 2018 Jan;167(1):195-203. doi: 10.1007/s10549-017-4432-0. Epub 2017 Sep 6. Breast Cancer Res Treat. 2018. PMID: 28879558 Free PMC article.
References
-
- Frable WJ. Surgical pathology--second reviews, institutional reviews, audits, and correlations: what’s out there? Error or diagnostic variation?Arch Pathol Lab Med 2006;130:620-5.pmid:16683875. - PubMed
-
- To Err is Human: Building a Safer Health System. National Academies of Sciences, Engineering, and Medicine, 2000. - PubMed
-
- Improving Diagnosis in Health Care. National Academies of Sciences Engineering, and Medicine, 2015.
-
- Hofvind S, Geller BM, Rosenberg RD, Skaane P. Screening-detected breast cancers: discordant independent double reading in a population-based screening program. Radiology 2009;253:652-60. 10.1148/radiol.2533090210 pmid:19789229. - DOI - PubMed
-
- Dinnes J, Moss S, Melia J, Blanks R, Song F, Kleijnen J. Effectiveness and cost-effectiveness of double reading of mammograms in breast cancer screening: findings of a systematic review. Breast 2001;10:455-63. 10.1054/brst.2001.0350 pmid:14965624. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical