

Sexual and physical abuse and gynecologic disorders
- PMID: 27334336
- PMCID: PMC4974667
- DOI: 10.1093/humrep/dew153
Sexual and physical abuse and gynecologic disorders
Abstract
Study question: Is sexual and/or physical abuse history associated with incident endometriosis diagnosis or other gynecologic disorders among premenopausal women undergoing diagnostic and/or therapeutic laparoscopy or laparotomy regardless of clinical indication?
Summary answer: No association was observed between either a history of sexual or physical abuse and risk of endometriosis, ovarian cysts or fibroids; however, a history of physical abuse was associated with a higher likelihood of adhesions after taking into account important confounding and mediating factors.
What is known already: Sexual and physical abuse may alter neuroendocrine-immune processes leading to a higher risk for endometriosis and other noninfectious gynecologic disorders, but few studies have assessed abuse history prior to diagnosis.
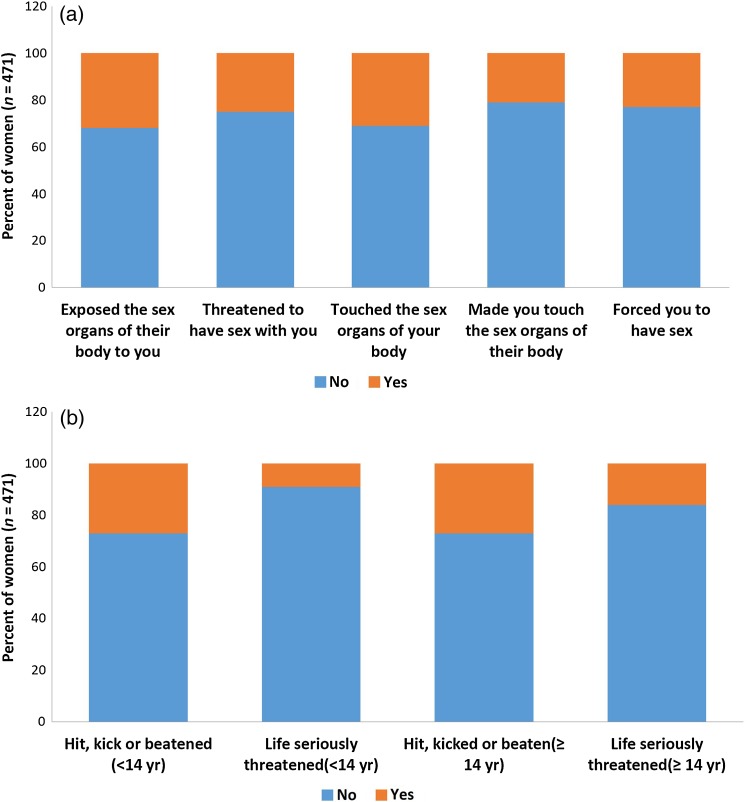
Study design, size, duration: The study population for these analyses includes the ENDO Study (2007-2009) operative cohort: 473 women, ages 18-44 years, who underwent a diagnostic and/or therapeutic laparoscopy or laparotomy at 1 of the 14 surgical centers located in Salt Lake City, UT, USA or San Francisco, CA, USA. Women with a history of surgically confirmed endometriosis were excluded.
Participants/materials, setting and methods: Prior to surgery, women completed standardized abuse questionnaires. Relative risk (RR) of incident endometriosis, uterine fibroids, adhesions or ovarian cysts by abuse history were estimated, adjusting for age, race/ethnicity, education, marital status, smoking, gravidity and recruitment site. We assessed whether a history of chronic pelvic pain, depression, or STIs explained any relationships via mediation analyses.
Main results and role of chance: 43 and 39% of women reported experiencing sexual and physical abuse. No association was observed between either a history of sexual or physical abuse, versus no history, and risk of endometriosis (aRR: 1.00 [95% confidence interval (CI): 0.80-1.25]); aRR: 0.83 [95% CI: 0.65-1.06]), ovarian cysts (aRR: 0.67 [95% CI: 0.39-1.15]); aRR: 0.60 [95% CI: 0.34-1.09]) or fibroids (aRR: 1.25 [95% CI: 0.85-1.83]); aRR: 1.36 [95% CI: 0.92-2.01]). Conversely, a history of physical abuse, versus no history, was associated with higher risk of adhesions (aRR: 2.39 [95% CI: 1.18-4.85]). We found no indication that the effect of abuse on women's adhesion risk could be explained by a history of chronic pelvic pain, depression or STIs.
Limitations, reasons for caution: Limitations to our study include inquiries on childhood physical but not sexual abuse. Additionally, we did not inquire about childhood or adulthood emotional support systems, found to buffer the negative impact of stress on gynecologic health.
Wider implications of the findings: Abuse may be associated with some but not all gynecologic disorders with neuroendocrine-inflammatory origin. High prevalence of abuse reporting supports the need for care providers to screen for abuse and initiate appropriate follow-up.
Study funding/competing interests: Supported by the Intramural Research Program, Eunice Kennedy Shriver National Institute of Child Health and Human Development (contracts NO1-DK-6-3428, NO1-DK-6-3427, and 10001406-02). The authors have no potential competing interests.
Keywords: endometriosis; epidemiology; pelvic adhesions; physical abuse; sexual abuse.
© The Author 2016. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures


References
-
- American Society for Reproductive Medicine. American College of Obstetricians and Gynecologists Committee Opinion No. 518: Intimate partner violence. Obstet Gynecol 2012;119:412–417. - PubMed
-
- American Society for Reproductive Medicine. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertil Steril 1997;67:817–821. - PubMed
-
- Beck AT, Steer RA, Brown GK. BDI-Fast Screen for Medical Patients: Manual. San Antonio, TX: The Psychological Corporation, 2000.
-
- Black MC, Basile KC, Breiding MJ, Smith SG, Walters ML, Merrick MT, Chen J, Stevens MR. The National Intimate Partner and Sexual Violence Survey (NISVS): 2010 Summary Report. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. http://www.cdc.gov/violenceprevention/pdf/nisvs_report2010-a.pdf (29 January 2016, date last accessed).
-
- Bonomi AE, Anderson ML, Rivara FP, Thompson RS. Health outcomes in women with physical and sexual intimate partner violence exposure. J Womens Health (Larchmt) 2007;16:987–997. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
