Preoperative Lymph Node Staging by FDG PET/CT With Contrast Enhancement for Thyroid Cancer: A Multicenter Study and Comparison With Neck CT
- PMID: 27334517
- PMCID: PMC5327587
- DOI: 10.21053/ceo.2015.01424
Preoperative Lymph Node Staging by FDG PET/CT With Contrast Enhancement for Thyroid Cancer: A Multicenter Study and Comparison With Neck CT
Abstract
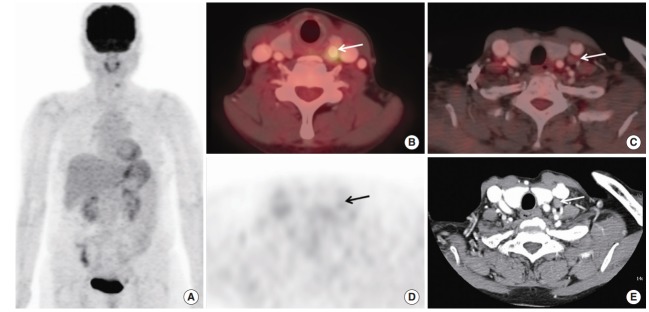
Objectives: The purpose of this study was to compare lymph node (LN) staging using 18F-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) with contrast-enhancement (CE) PET/CT and contrast-enhanced neck CT (neck CT) in patients with thyroid cancer with level-by-level comparison with various factors.
Methods: This was a retrospective multicenter study. A total of 85 patients were enrolled. Patients who underwent a preoperative evaluation by CE PET/CT and neck CT for thyroid cancer were enrolled. The gold standard for LN was the combination of surgical pathology and clinical follow-up. We compared CE PET/CT with neck CT using a level-by-level method. Factors, including age, sex, camera, arm position, tumor size, extra-thyroidal extension, tumor location, number of primary tumors, primary tumor maximum standardized uptake value, and the interval from scan to operation were also analyzed.
Results: Overall accuracy was 81.2% for CE PET/CT and 68.2% for neck CT. CE PET/CT was more sensitive than neck CT (65.8% vs. 44.7%). Also, CE PET/CT showed higher negative predictive value (77.2% vs. 66.1%). CE PET/CT showed good agreement with the gold standard (weighted kappa [κ], 0.7) for differentiating N0, N1a, and N1b, whereas neck CT showed moderate agreement (weighted κ, 0.5). CE PET/CT showed better agreement for the number of levels involved with the gold standard (weighted κ, 0.7) than that of neck CT with the gold standard (weighted κ, 0.5). The accuracies for differentiating N0, N1a, and N1b were 81.2% for CE PET/CT and 68.2% for neck CT. Level-by-level analysis showed that CE PET/CT was more sensitive and has higher negative predictive value for detecting ipsilateral level IV and level VI LNs than neck CT. Other analyzed factors were not related to accuracies of both modalities.
Conclusion: CE PET/CT was more sensitive and reliable than neck CT for preoperative LN staging in patients with thyroid cancer.
Keywords: Computed Tomography; Fluorodeoxyglucose F18; Positron-Emission Tomography; Thyroid Neoplasms.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Integrated analysis of 18F-FDG PET/CT improves preoperative lymph node staging for patients with invasive bladder cancer.Eur Radiol. 2019 Aug;29(8):4286-4293. doi: 10.1007/s00330-018-5959-0. Epub 2019 Jan 21. Eur Radiol. 2019. PMID: 30666449
-
Comparison of FDG PET/CT and MRI in lymph node staging of endometrial cancer.Ann Nucl Med. 2016 Feb;30(2):104-13. doi: 10.1007/s12149-015-1037-8. Epub 2015 Nov 6. Ann Nucl Med. 2016. PMID: 26546334
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Diagnostic role of F-18 FDG PET/CT for preoperative lymph node staging in thyroid cancer patients; A systematic review and metaanalysis.Clin Imaging. 2020 Sep;65:100-107. doi: 10.1016/j.clinimag.2020.04.030. Epub 2020 Apr 25. Clin Imaging. 2020. PMID: 32387798
-
Diagnostic accuracy of F-18 FDG PET or PET/CT for detection of lymph node metastasis in clinically node negative head and neck cancer patients; A systematic review and meta-analysis.Am J Otolaryngol. 2019 Mar-Apr;40(2):297-305. doi: 10.1016/j.amjoto.2018.10.013. Epub 2018 Oct 23. Am J Otolaryngol. 2019. PMID: 30473166
Cited by
-
Diagnostic values of F-18 FDG PET or PET/CT, CT, and US for Preoperative Lymph Node Staging in Thyroid Cancer: A Network Meta-Analysis.Br J Radiol. 2021 Apr 1;94(1120):20201076. doi: 10.1259/bjr.20201076. Epub 2021 Feb 17. Br J Radiol. 2021. PMID: 33595337 Free PMC article.
-
The Use of 18F-FDG PET/CT in Patients with Recurrent Differentiated Thyroid Cancer.Mol Imaging Radionucl Ther. 2021 Oct 15;30(3):137-143. doi: 10.4274/mirt.galenos.2021.02360. Mol Imaging Radionucl Ther. 2021. PMID: 34658228 Free PMC article.
-
Prediction of cervical metastasis and survival in cN0 oral cavity cancer using tumour 18F-FDG PET/CT functional parameters.J Cancer Res Clin Oncol. 2020 Dec;146(12):3341-3348. doi: 10.1007/s00432-020-03313-8. Epub 2020 Jul 8. J Cancer Res Clin Oncol. 2020. PMID: 32642973 Free PMC article.
-
Risk factors of malignant fluorodeoxyglucose-avid lymph node on preablation positron emission tomography in patients with papillary thyroid cancer undergoing radioiodine ablation therapy.Medicine (Baltimore). 2019 Apr;98(16):e14858. doi: 10.1097/MD.0000000000014858. Medicine (Baltimore). 2019. PMID: 31008921 Free PMC article.
-
Diagnostic performance of CT in detection of metastatic cervical lymph nodes in patients with thyroid cancer: a systematic review and meta-analysis.Eur Radiol. 2019 Sep;29(9):4635-4647. doi: 10.1007/s00330-019-06036-8. Epub 2019 Feb 26. Eur Radiol. 2019. PMID: 30806803
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012 Jan-Feb;62(1):10–29. - PubMed
-
- Adam MA, Pura J, Goffredo P, Dinan MA, Reed SD, Scheri RP, et al. Presence and number of lymph node metastases are associated with compromised survival for patients younger than age 45 years with papillary thyroid cancer. J Clin Oncol. 2015 Jul;33(21):2370–5. - PubMed
-
- Stack BC, Jr, Ferris RL, Goldenberg D, Haymart M, Shaha A, Sheth S, et al. American Thyroid Association consensus review and statement regarding the anatomy, terminology, and rationale for lateral neck dissection in differentiated thyroid cancer. Thyroid. 2012 May;22(5):501–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources